Description of Radial Endobronchial Ultrasound Miniature Probes (EBUS) in Pulmonary Medicine
Author: Prof. Felix JF Herth, MD, PhD, DSc, Thoraxklinik, University of Heidelberg, Germany Source: DVD-ROM ‘Endoscopic Ultrasound – Diagnostics and Staging of Lung Cancer’, Olympus Europa SE & Co. KG, 2013
Improving Diagnostics of the Airways

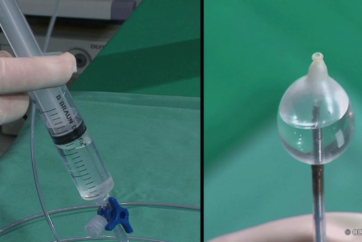
For application inside the airways, Olympus developed radial endobronchial ultrasound miniature probes (EBUS), catheters as well as catheters with a balloon at the tip that allow circular contact also in the larger lumen. Radial EBUS probes provide a complete 360° image of the parabronchial structures and under favourable conditions visualise structures up to a distance of 4 cm.

Peripheral Lesions (SPN)
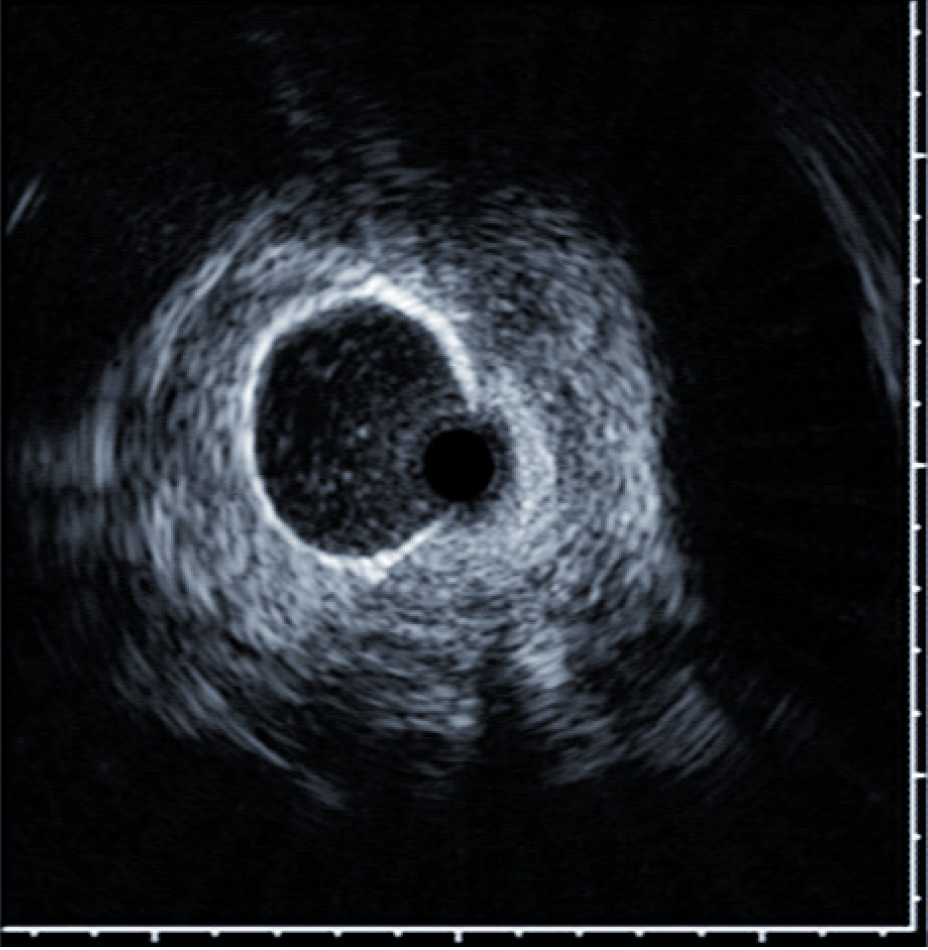
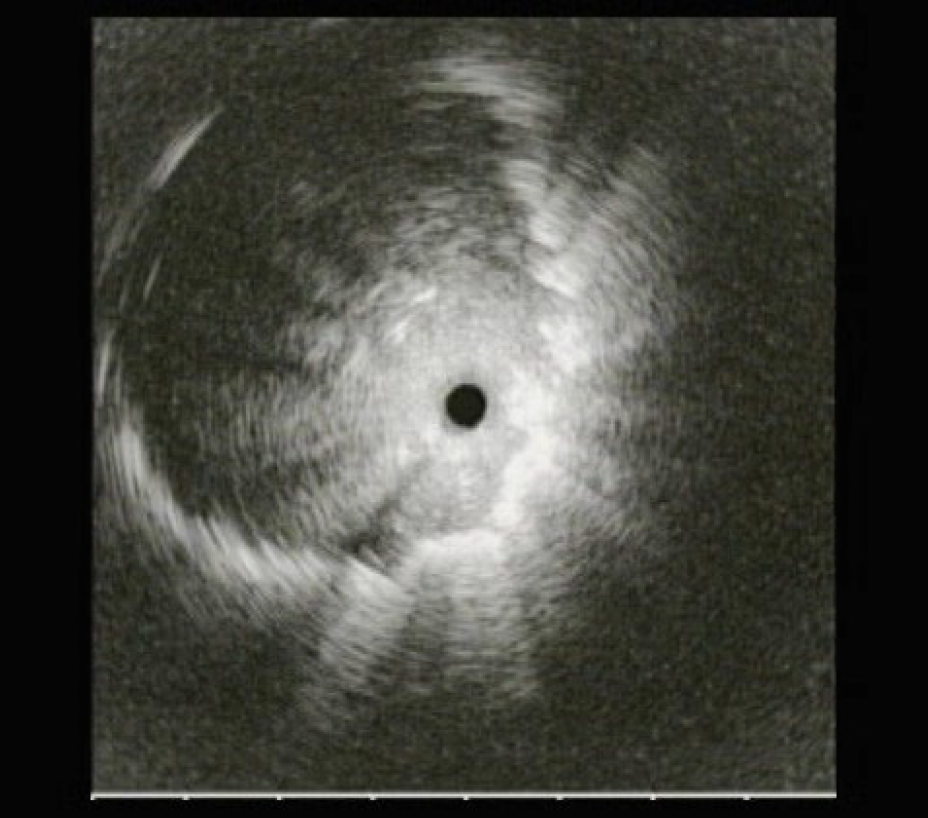
Solitary pulmonary nodules are an increasing diagnostic problem. Multiple approaches may be undertaken to establish a tissue diagnosis, including sputum cytology, percutaneous image-guided aspiration/biopsy, and bronchoscopic sampling. To obtain tissue samples for the histological evaluation of peripheral lesions, bronchoscopy under fluoroscopy is the standard procedure. This demands expensive x-ray equipment in the bronchoscopy suite or coordination with the radiology department and causes exposure to radiation for patient and staff. An important factor affecting the yield is that lesions situated beyond the airway lumen are not visible to the bonchoscopist, resulting in ‘blind’ biopsies. Fluoroscopy offers some assistance for localizing such lesions, especially in lesions larger than 3 cm. The two-dimensional projection views produced by fluoroscopy often do not show smaller lesions. In such lesions, mostly peripheral pulmonary lesions not visible endobronchially, diagnostic yield of routine bronchoscopy may therefore be less than 20%. The highest diagnostic yield for bronchoscopic evaluation of small SPNs appears to be associated with the use of radial ultrasound miniature probes (EBUS) in the diagnostic procedure. EBUS miniature probes employ a flexible catheter, housing a mechanically rotated ultrasound transducer which produces a 360° radial ultrasound image. The technique to use a miniature probe to guide TBLB was first described by Herth (Herth et al, Endobronchial Ultrasound-Guided Transbronchial Lung Biopsy in Solitary Pulmonary Nodules and Peripheral Lesions, Eur Respir J., 2002, Oct; 20(4), pp 972- 974) passing the probe into the bronchial subsegments until the characteristic ultrasound signal of a solid lesion is displayed. Numerous groups have published their experience with EBUS-guided evaluation of SPNs since.


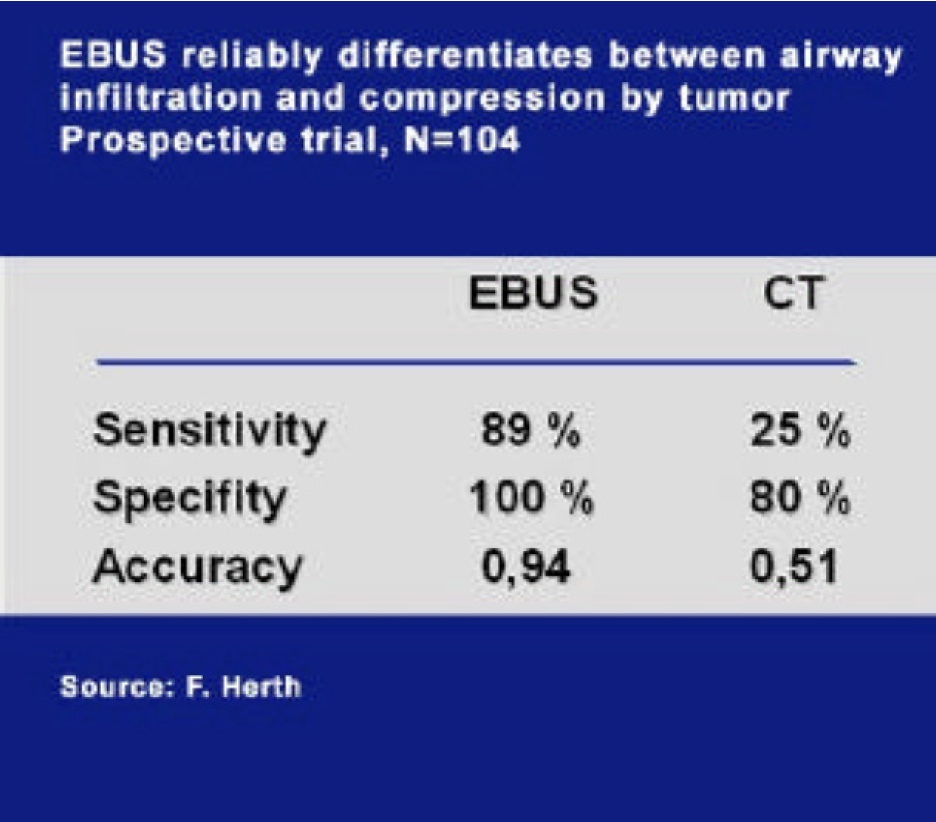
Invasion vs. Compression
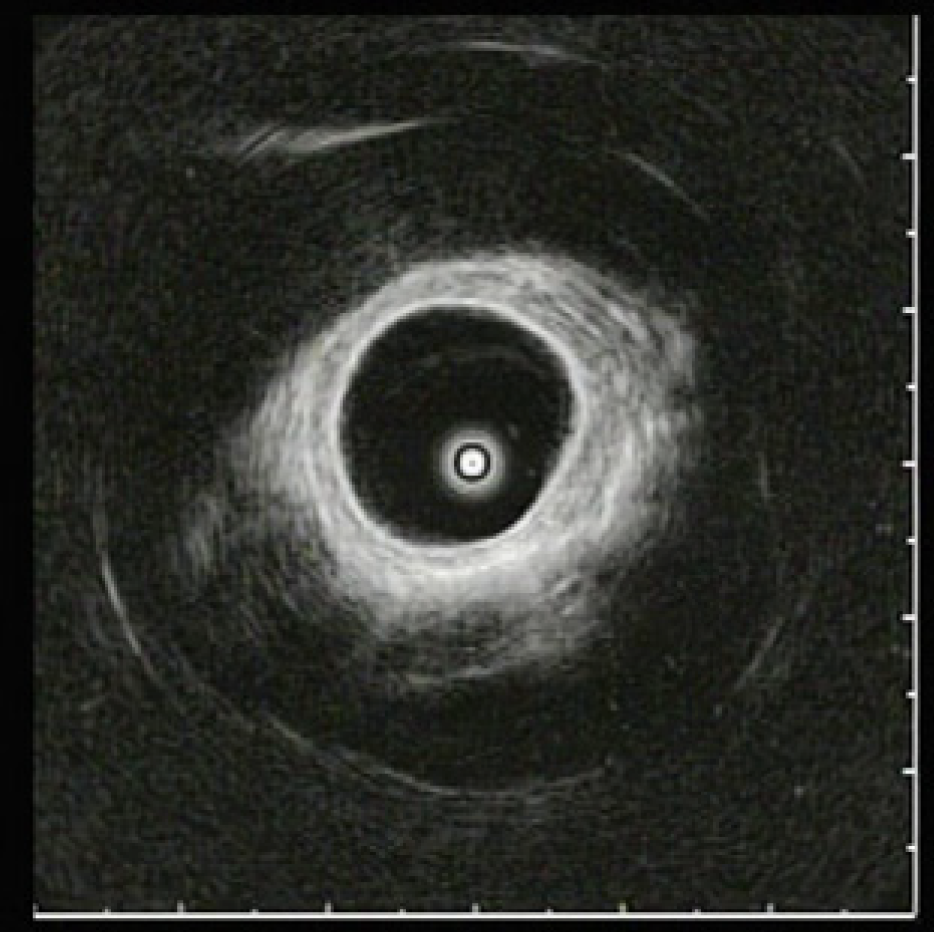
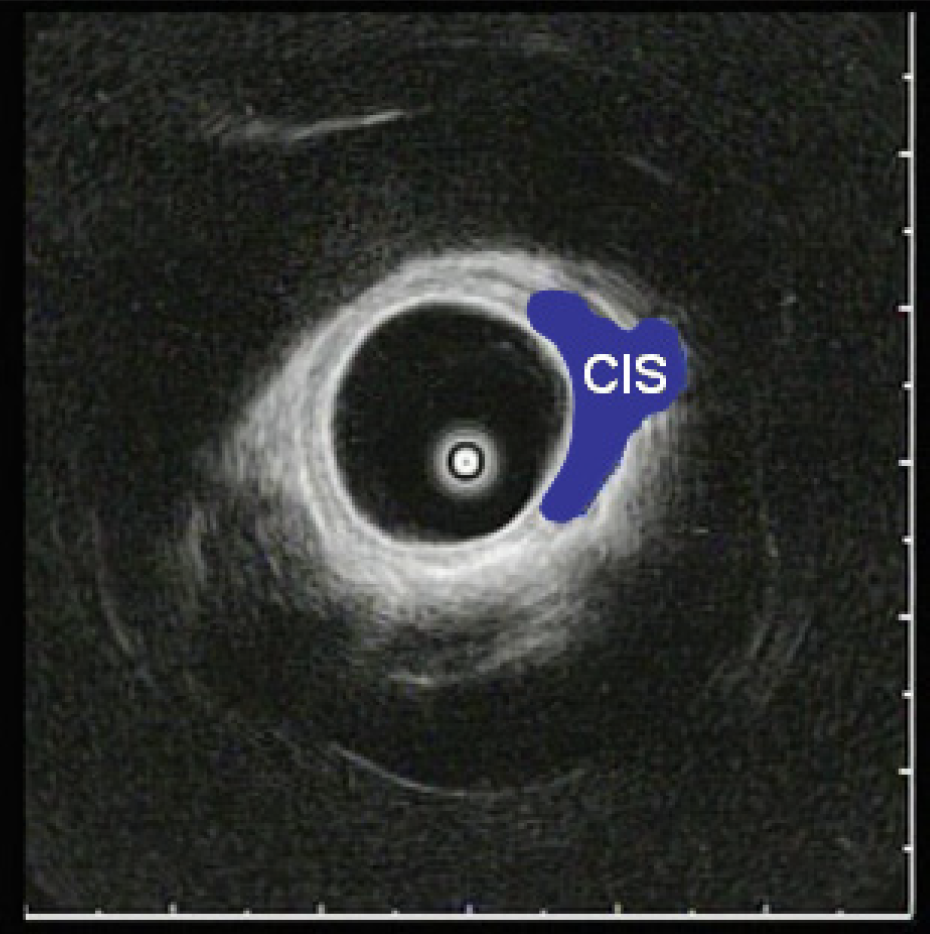
Early Cancer / CIS
Conclusion
EBUS miniature probes have proven to be extremely useful. In many instances EBUS was superior for T-staging of lung cancer and for the diagnostics of other pathologies. EBUS is a valuable tool, especially for on-the-spot decision making during diagnostic and interventional procedures. With regards to the technique in clinical application and diagnostic results, radial endobronchial ultrasound is a routine procedure.
- Keyword
- Content Type