Colorectal ESD

Dr. Yuichiro Yamaguchi, Division of Endoscopy, Shizuoka Cancer Center
Dr. Yuichiro Yamaguchi works in the Division of Endoscopy at the Shizuoka Cancer Center with Dr. Ono. Regarding the importance of selecting the right device, Dr. Yamaguchi explains the features, benefits and the usage of ITknife nano for colorectal ESD.
ITknife nano, a suitable knife for colorectal ESD
What are the benefits of using the ITknives?
The range of incision and dissection per stroke is proportional to the area of the knife. Because the ITknives have a wider knife area than needle-type knives, dissection becomes faster, helping to reduce the procedure time.
Another advantage of the ITknife range is its insulated tip. Customers using needle-type knives must always take the distance of the current into consideration and manipulate the knife; otherwise, they may result in perforation. The risk is higher in the colon where it has many bends and folds and using a needle-type knife without being able to confirm the muscle layer can lead to perforation. Using ITknife nano can minimize the perforation risk since it is possible to predict the incision or dissection point due to the insulated tip.
A precise control capability of ITknife nano
Though the current ITknives also have an insulated tip, it is too big and the knife length is too long to manipulate in organs with a narrow lumen. For these reasons, I believe it is difficult to take full advantage of these applications using the current ITknife.
ITknife nano resolves these issues due to the fact that the minimized insulated tip enables precise knife contact with the tissue. The knife length has been reduced to 3.5 mm to make it easier to manipulate in a restricted working space, significantly improving manipulation capability in colorectal ESD.
ITknife nano with horizontal and vertical dissection capabilities
Due to the small disc-shaped electrode on the back of the insulated tip, ITknife nano can be used to perform a “hooking cut” by pulling the whole knife toward the proximal side to cut the tissue that is in contact with the disc-shaped electrode and long blade. (Fig.1)
Incision and dissection with ITknife nano generally requires the knife to be moved in the lateral direction. However, if this is not possible, moving the knife toward the proximal side by utilising the disc-shaped electrode and long blade makes it possible to dissect the tissue in a vertical direction.
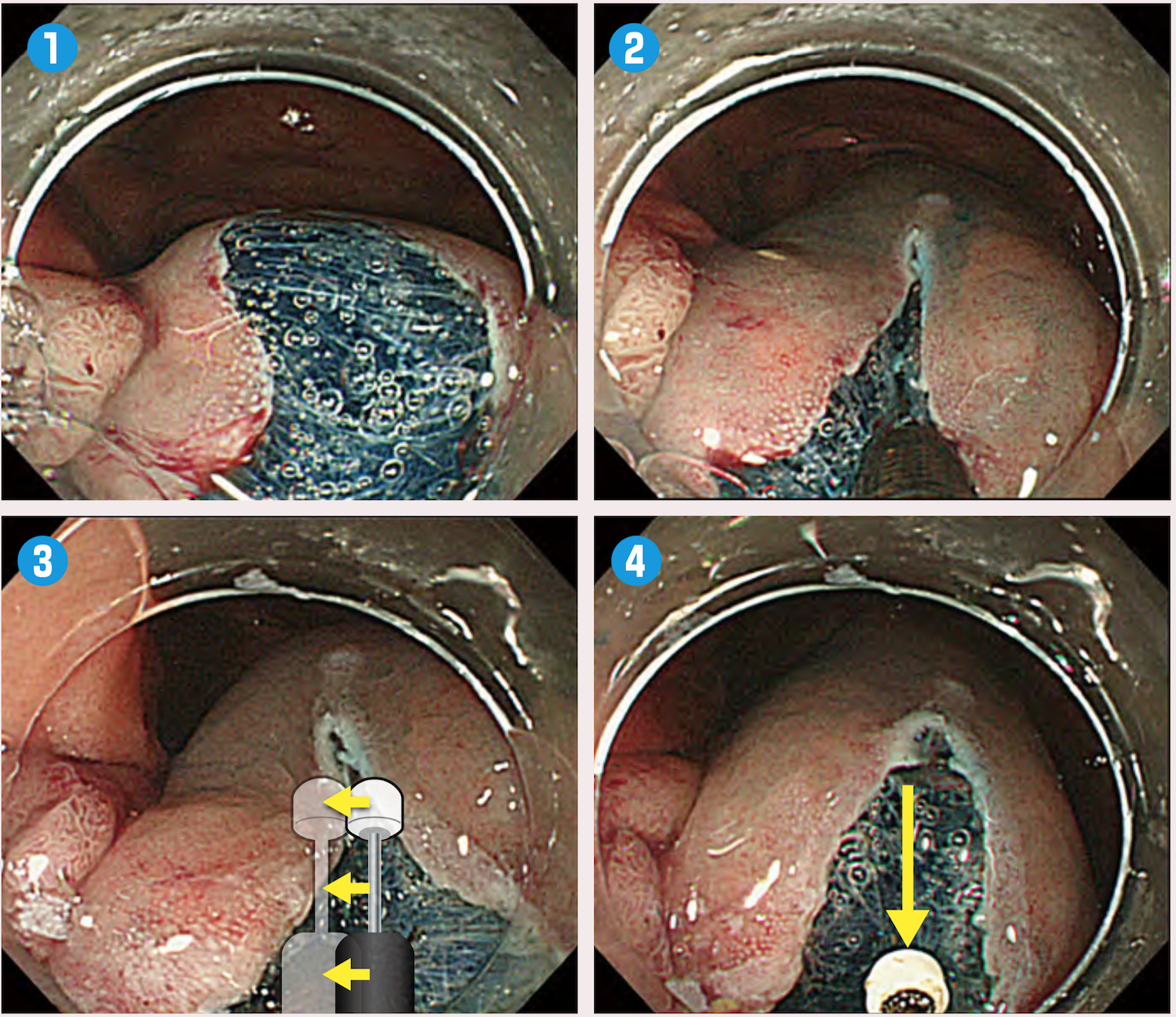
Fig.1:“Hooking cut” using ITknife nano
“Hooking cut” is used when horizontal manipulation is difficult. Contact the long blade with the submucosal tissue you want to dissect. Pull the device toward the proximal side and you can perform dissection using the disc-shaped electrode and long blade. While not moving the knife more than it is in contact with the tissue, pull the device toward the proximal side.Suitable cutting ability for Colorectal ESD
Some customers who are used to ITknife2 may feel that the cutting ability of ITknife nano is inadequate when used in the same environment such as in gastric ESD. It is important for these doctors to understand that these features were deliberately designed so that it can be used in organs with thin walls.
ITknife nano has its own manipulation methods, and new users will need to adapt to them.
Tips on using ITknife nano in colorectal ESD
Utilize the insulated tip for stable endoscope manipulation
The degree of safe colorectal ESD is determined by the stability of endoscope manuevrability. Since the colon moves, it is critical to stabilize the endoscope and fix it on the target point. The movement of the colon comes from the intestinal rotation caused by insertion of the endoscope, heartbeat and respiratory fluctuation. Decisions regarding colorectal ESD should be based on accurate identification of endoscope movement. Patients under sedation tend to move more because they often breathe deeper. When a needle-type knife is used in areas where the colon tends to move, incision or dissection must be performed while the distal end of the endoscope is not in contact with the intestinal wall. On some occasions it may be necessary to wake the patient up from sedation and have them hold their breath or retroflex the endoscope and apply it against the intestinal wall to stabilize the distal end of the endoscope.As the tip of ITknife nano is insulated, it is possible to reduce the movement of the intestinal tract movement by applying the insulated tip to the tissue to fix the endoscope. Since the endoscopic image does not fluctuate even when the endoscope is not retroflexed(this may be due to the synchronization of the endoscope’s movement with the colon), colorectal ESD can be performed more stably than when a needle-type knife is used due to the improved field of view.

How to approach the submucosal layer
The mucosal layer of the colon is so soft that it tends to act like pleated bellows even when tension is applied with the long blade making it difficult to perform a circumferential incision. For this reason, it is required to incise the mucosa by applying the long blade gently to the mucosa and then applying tension. (Fig.2)
For submucosal dissection, it is important to incise the mucosa accurately down to the muscularis mucosae. The point of this step is to slightly straighten the position of the knife in order to prevent the spark that is discharged from the disc-shaped electrode damaging the muscle layer.
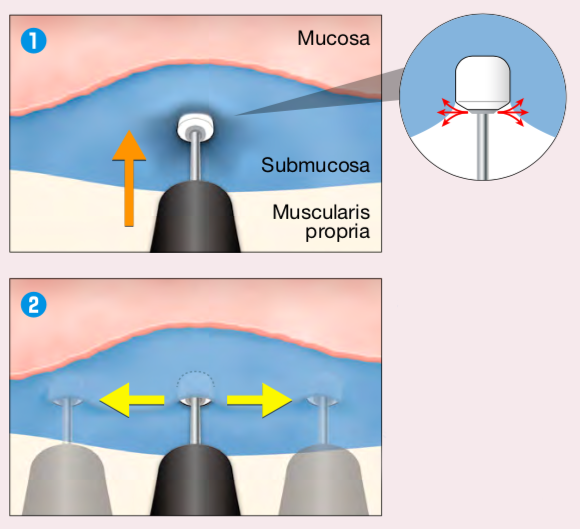
Fig.2:“Press cut”
“Press cut” is used when it is difficult to find the starting point for dissection. Press the insulated tip towards the submucosal layer and use the side spark of the disc-shaped electrode to make a starting point.Perform dissection little by little
The dissection technique of gastric ESD and colorectal ESD differs. The basic dissection technique in gastric ESD is to slide the long blade of ITknife2 just above the muscle layer. Since the colonic mucosa is thinner, the blade of ITknife nano should be advanced through the middle layer of the submucosa.(Fig.3) In addition, as the colonic mucosa is softer than the gastric mucosa, dissecting the tissue by hooking it with the long blade like in gastric ESD would catch the muscle layer. To avoid this, I dissect the tissue little by little as I would with the needle-type knife and confirm that the tissue in front has been dissected before proceeding to the next dissection. Even with ITknife nano, it is unsafe to dissect the colonic tissue in the same way one would for gastric ESD.
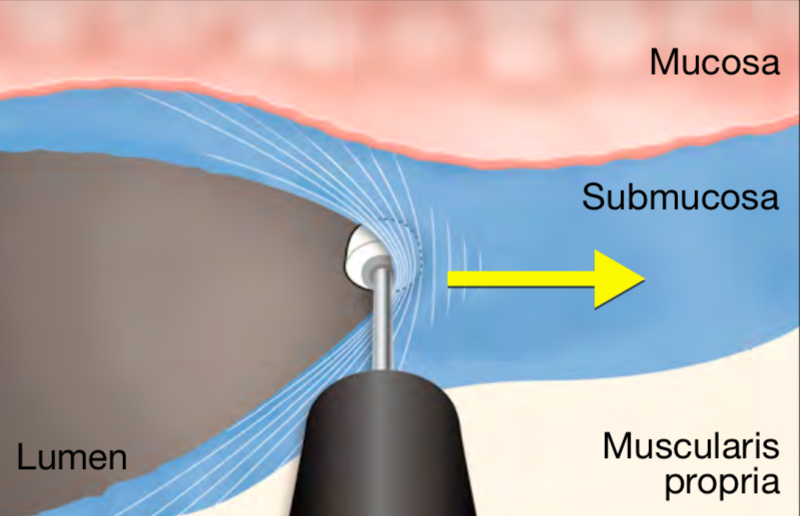
Fig.3:Dissection of colorectal ESD
The basic dissection technique in gastric ESD is to slide the long blade of ITknife2 just above the muscle layer. Since the colonic mucosa is thinner, the blade of ITknife nano should be advanced through the middle layer of the submucosa.Select a device according to the situation
The ITknife range requires a certain amount of skill to manipulate. However, once you get accustomed to them, they can be much more useful and versatile than other devices. Compared to ITknife2, ITknife nano can cut more precisely due to its minimized knife area. Since ITknife2 has a wide knife area compared to other knives, its impedance is small and requires a higher current setting. A higher setting may result in damaging the muscle layer with unintentional spark. ITknife nano’s blade is not as large as ITknife2’s so it is very effective in colorectal ESD due to its fine cutting capability. Although colorectal ESD has much in common with gastric ESD, a physician learning colorectal ESD should not rely on what they know about gastric ESD and practice the unique techniques for using ITknife nano in colorectal ESD. I believe this is the fastest way to learn how to perform safe colorectal ESD. Nevertheless, if the approach is difficult and the endoscopist judges that full incision as deep as the muscularis mucosal layer is not possible, it is recommended to switch to a needle-type knife. Since the final goal is a safe and secure resection, always use whichever device is most suitable in the circumstances.
Setting
| Electrosurgical unit | Treatment | Setting |
|---|---|---|
| VIO 300D | Mucosal Incision | EndoCutQ, Effect3, Cut Duration2, Cut Interval2 |
| Submucosal Dissection | SwiftCoag, Effect3, 30-40W* |
*For beginners, starting from 30W is recommended.
- Content Type