—S8 subsegmentectomy of the liver—
Dr. Keiichi Kubota, Second Department of Surgery, Dokkyo Medical University Hospital
Biography
Graduated from the School of Medicine, the Faculty of Medicine, The University of Tokyo in 1981. Entered the Second Department of Surgery, The University of Tokyo in 1985, after training in the surgical departments of The University of Tokyo Hospital, the Tokyo Metropolitan Police Hospital and other institutions. In 1988, moved to the Department of Transplantation Surgery, Karolinska Institute (Sweden). Since 1996, lecturer at the Department of Hepatobiliary and Pancreatic Surgery, The University of Tokyo. Since 2000, served as Professor and Chairman of the Second Department of Surgery, Dokkyo Medical University.
Qualifications: Medical instructor for the Japan Surgical Society, the Japanese Society of Gastroenterological Surgery, and the Japanese Society of Gastroenterology. A board certified instructor (Hepatobiliary-Pancreatic field).
Characteristics and points for use of THUNDERBEAT Open Extended Jaw/ electrosurgical generator ESG-400 in laparotomic hepatectomy
THUNDERBEAT has a Seal & Cut mode, which facilitates superior coagulation-hemostasis and rapid tissue incision by simultaneous output of bipolar and ultrasonic energy. It also has a Seal mode, which achieves sealing-hemostasis by emission of bipolar energy alone. In particular, the THUNDERBEAT Open Extended Jaw allows rapid hemostasis-incision of the liver parenchyma in a single action, and is expected to achieve superior sealing for small branches of the hepatic vein. In fact, it can be used in both superficial and deep portions of the liver parenchyma. In addition, it is characterized by a light grip that allows high compression to be applied. This model incorporates a new function whereby the energy output stops automatically at completion of tissue dissection. This is expected to improve the durability of the tissue pad.
In addition, the electrosurgical generator ESG-400 (Soft Coag mode) is characterized by absence of discharge at low voltage and reduced carbonization of the tissue, resulting in secure and safe hemostasis. In fact, effective hemostasis was achieved for bleeding from the liver parenchyma and bleeding from the ostium of the hepatic vein. Moreover, the depth of penetration can be adjusted by the effect setting. Therefore, it is important to use it to adjust the depth of penetration appropriately so that effective hemostasis to control bleeding from the liver parenchyma can be achieved. Provided the characteristics of the THUNDERBEAT Open Extended Jaw/electrosurgical generator ESG-400 are fully understood, hepatectomy can be performed rapidly and safely.

Points regarding laparotomic hepatectomy performed at our hospital
After laparotomy with a J-shaped or L-shaped incision, in the case of resection of the posterior segment and S8, right thoracotomy is carried out to secure a good visual field for hepatectomy. If the ICG 15-minute retention rate is less than 30%, systematic resection is performed as much as possible. Especially, S8 segmentectomy is a highly difficult procedure due to large resection volume and the need to expose the right and middle hepatic veins. In the present report, hepatectomy using THUNDERBEAT Open Extended Jaw/electrosurgical generator ESG-400 (hereinafter THUNDERBEAT) is described.
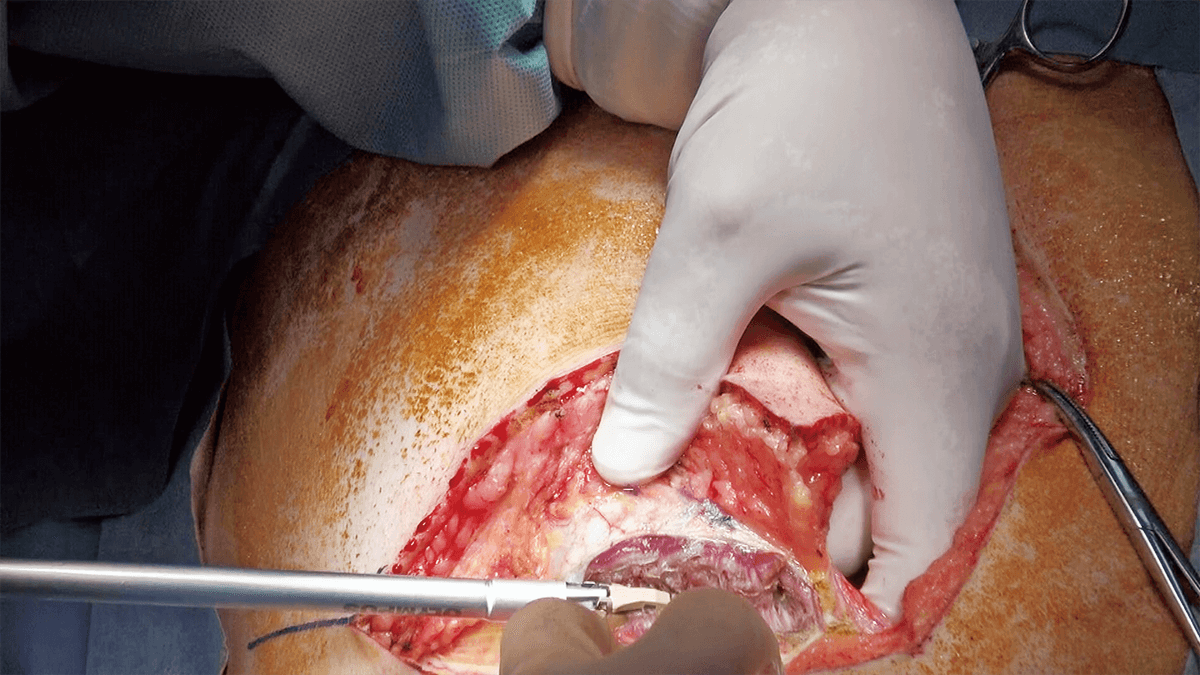
Skin incision and laparotomy-thoracotomy/detachment of ligaments and mobilization
Laparotomy-thoracotomy is performed by making a J-shaped incision consisting of a median incision from the xiphoid process to two fingerbreadths above the umbilicus and an additional oblique incision toward the ninth intercostal space. THUNDERBEAT proved to be effective in muscle dissection demonstrating a superior hemostasis effect (Figure 1). A good visual field can be obtained by retracting the costal arch and the left abdominal wall using a Kent retractor (Figure 2). Since thoracotomy has already been done, only minimal detachment of ligaments is required because a sufficient visual field can be obtained by inserting a hand into the right thoracic cavity to lift the liver.

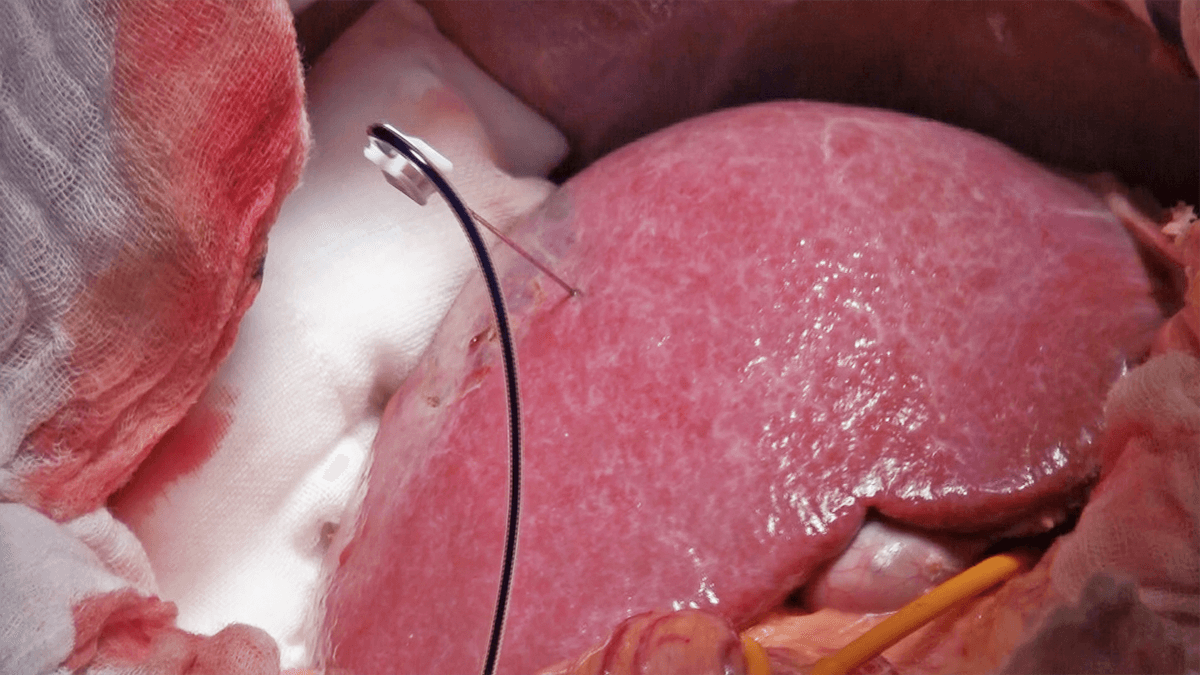
Determination of the range of dissection-dissection of the liver parenchyma
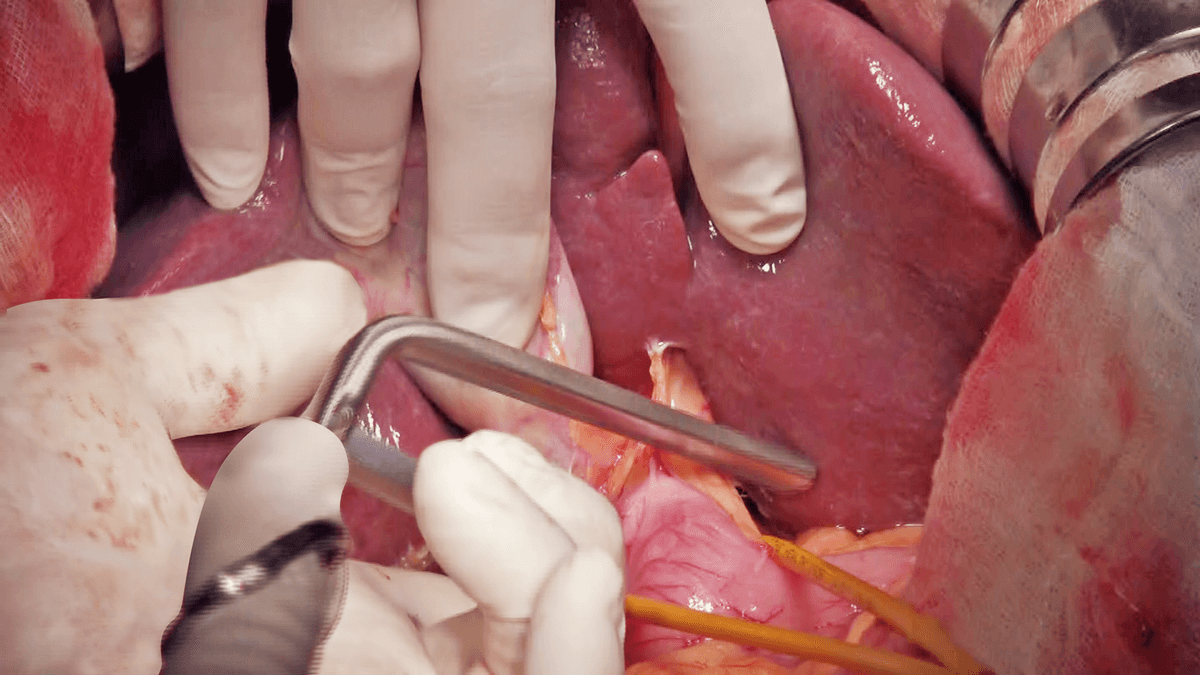
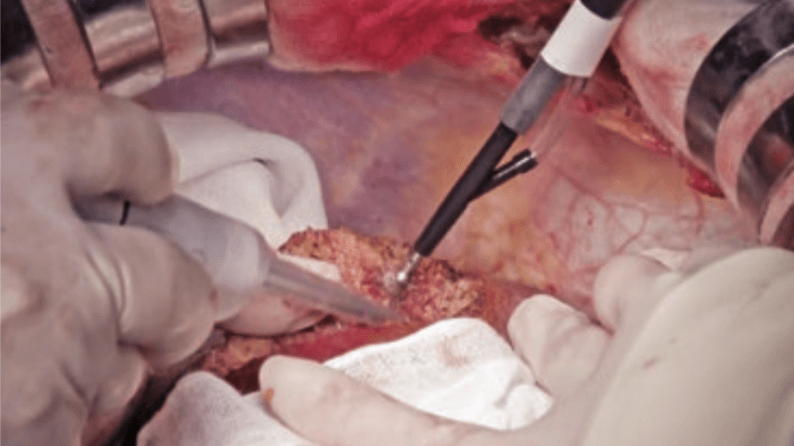
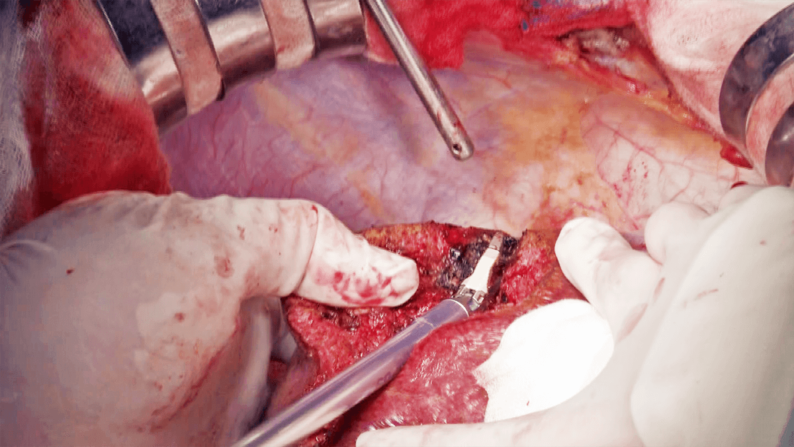
After puncture of P8 under intraoperative ultrasound guidance and injection of 5 mL of indigo carmine, the stained region is marked by electrosurgical generator (Figure 3). The liver parenchyma is dissected under total hepatic ischemia created by blocking blood flow for 15 minutes and releasing it for 5 minutes. After clamping the hepatoduodenal ligament with a Fogarty clamp and reducing the tidal volume (Figure 4), dissection of the liver parenchyma is started from the border between S5 and S8, and continued at the border between S8 and the medial segment and then at the border between S8 and S7.
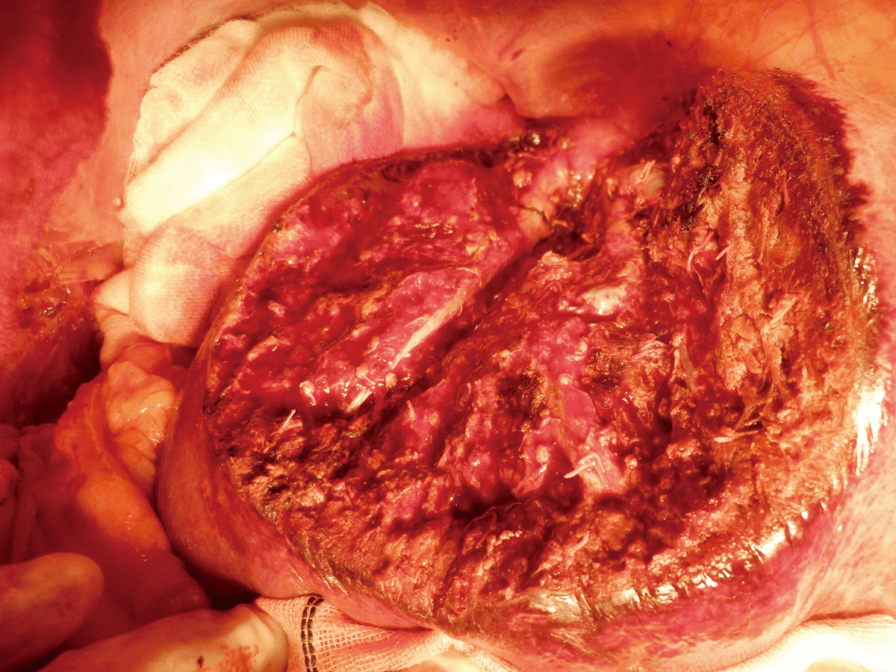
First, after slight crushing and aspirating the liver parenchyma along the marking line using CUSA, dissection is started using the Seal & Cut mode by grasping the liver parenchyma with the tissue pad of THUNDERBEAT (Figure 5). Bleeding from the liver parenchyma is stopped using the Soft Coag mode (Figure 6). When dissection proceeds to a somewhat deeper layer of the parenchyma, the liver parenchyma is lightly crushed with the tip; a technique referred to as the Pean fracture method, and dissection is continued while checking for the absence of vessels that need to be ligated (Figure 7). Upon reaching a deeper layer, the cord-like structure is ligated and dissected by combining CUSA and the Pean fracture method (Figure 8), or dissected by THUNDERBEAT if vessels are not identified. If the peripheral part of the middle hepatic vein is identified, the vein is carefully separated and exposed while dissecting toward the central direction, and small branches are dissected using the Seal & Cut mode. When P8 is identified, it is dissected with triple ligation. Dissection proceeds along the cranial surface of the Glisson’s sheath of the anterior segment. The border with S7 is dissected in a similar way, and the right hepatic vein is exposed using CUSA (Figure 9). Dissection proceeds toward the central side of the hepatic vein, the inferior vena cava is partially exposed, and S8 subsegmentectomy is completed (Figure 10).



After resection of the specimen
Sufficient hemostasis is obtained, and the absence of bile leakage is verified. A drain is inserted into the thoracic cavity and another into the dissection plane. The wound is closed to complete the surgery.
Summary
Hepatectomy with minimal bleeding by decreasing CVP through reduction of the tidal volume under clamping of the hepatoduodenal ligament and by using the THUNDERBEAT for dissection of the liver parenchyma could be performed.
Experience of the clinical use of Intelligent Tissue Monitoring (ultrasonic output control technology)
The earlier model of THUNDERBEAT would on occasions become unusable during surgery requiring long surgical times and the use of many devices, etc., because the tissue pad was easily worn away.
In patients treated with the newly incorporated output control function, surgery could be completed successfully because the automatic arrest worked to some degree and there was no damage to the device. It was found to be especially effective where visibility of the tip was poor during dissection of the liver parenchyma. Although this function does not work for all outputs because the arrest occurs with a short delay after completion of dissection, it should be of assistance, especially for young doctors.
Frequency of clinically detected cases
| Surgical procedure | Frequency of output | Frequency of ITM detection |
| Skin incision (rectus abdominis muscle incision) | 18 | 6 (33%) |
| Cholecystectomy + treatment of the hepatic portal region | 3 | 1 (33%) |
| Mobilization of the liver (dissection of ligaments) | 35 | 4 (11%) |
| Superficial dissection of the liver | 22 | 20 (91%) |
| Deep dissection of the liver | 28 | 16 (57%) |


Site profile
Since its establishment in Mibu-machi, Tochigi prefecture on July 14, 1974, Dokkyo Medical University Hospital is the main center of community medicine (number of beds: 1,167) designated as an advanced treatment hospital. It is also a core emergency medicine center equipped with helicopter ambulances. The Second Department of Surgery, where 130-140 hepatectomy procedures and 60-70 pancreatectomy procedures are performed a year, is certified as a board certified training institution A (Hepatobiliary-Pancreatic field).
- Keyword
- Content Type