Procedure Steps
Disclaimer
This surgical technique is presented to demonstrate the technique utilized by Prof. Raßler, MD of the Urology Department at the St. Elisabeth Hospital in Leipzig (Germany).
Olympus as manufacturer does not practice medicine, and therefore the information on the products and procedures contained in this document is of a general nature and does not represent and does not constitute medical advice or recommendations. This information does not purport to constitute any diagnostic or therapeutic statement with regard to any individual medical case. Each patient must be examined and advised individually, and this document does not replace the need for such examination and/or advice in whole or in part.
Please refer to the instructions for use for important product information, including, but not limited to, contraindications, warnings, precautions, and adverse effects.
01 | Cystoscopy with Inspection of Urethra
Inspection of the Urethra and Bladder.
Inspect left and right ostium, bladder, verumontanum, internal and external sphincter.
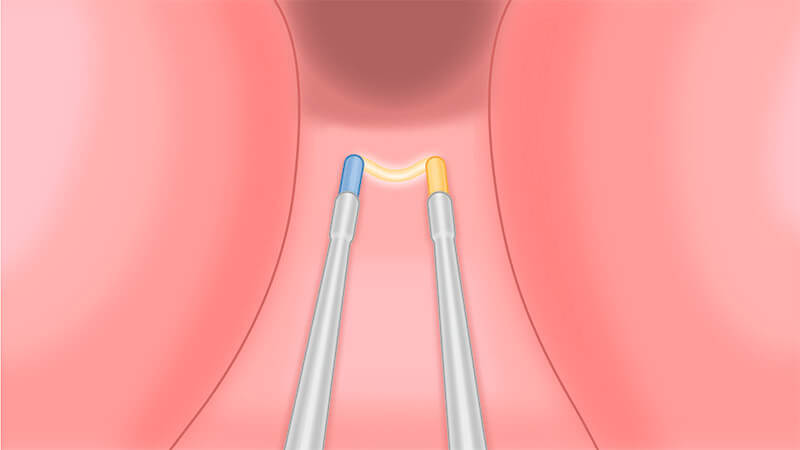
02 | Marking of Resection Borders
Proximal Marking of Verumontanum in EP Procedures.

Use the coagulation mode of the loop to superficially mark the resection borders at a distance of approximately two loops from the verumontanum.
03 | Resection of Irrigation Channel at 6 O’Clock Position or of Medial Prostate Lobe
Plasma Resection of Irrigation Channel or, if Present, Complete Resection of the Medial Lobe.
Resection at 6 o’clock position starting at the bladder neck down to the borders of resection.
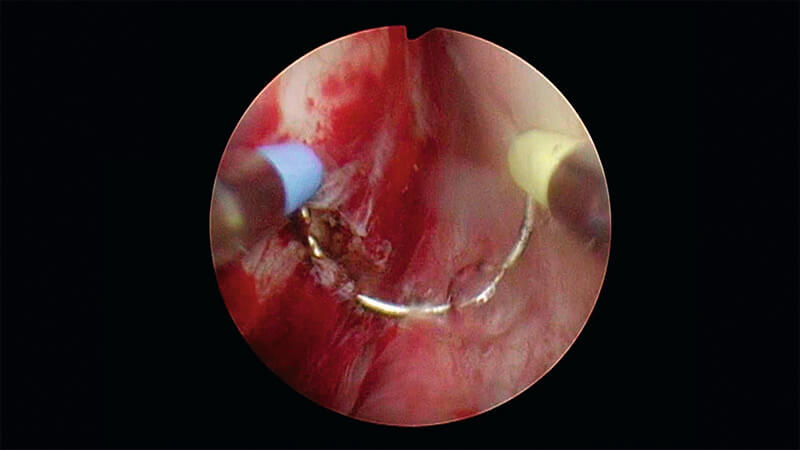
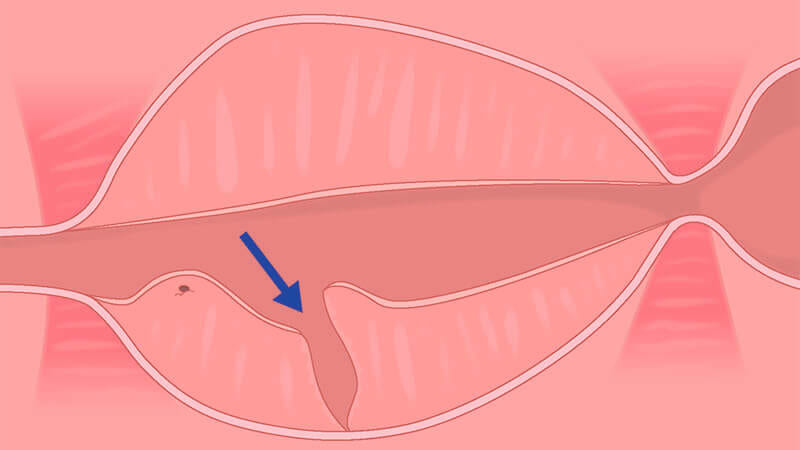
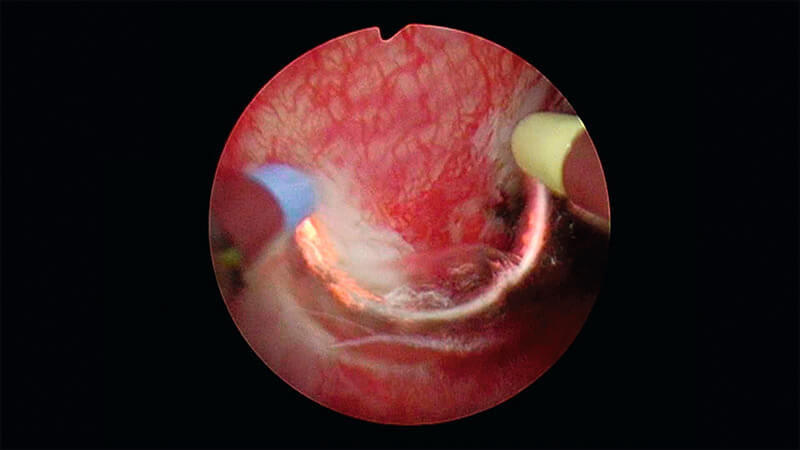
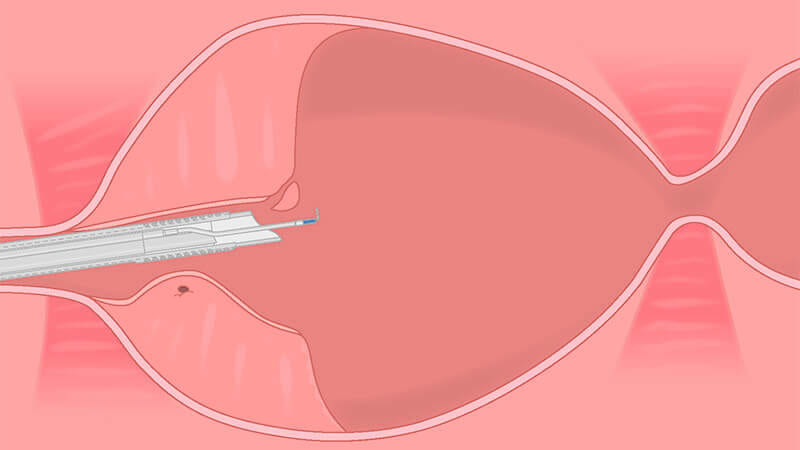
04 | Initiation of Enucleation of the Left Prostate Lobe
Paracollicular Prograde Incision with Plasma of the Mucosa of the Left Lobe.
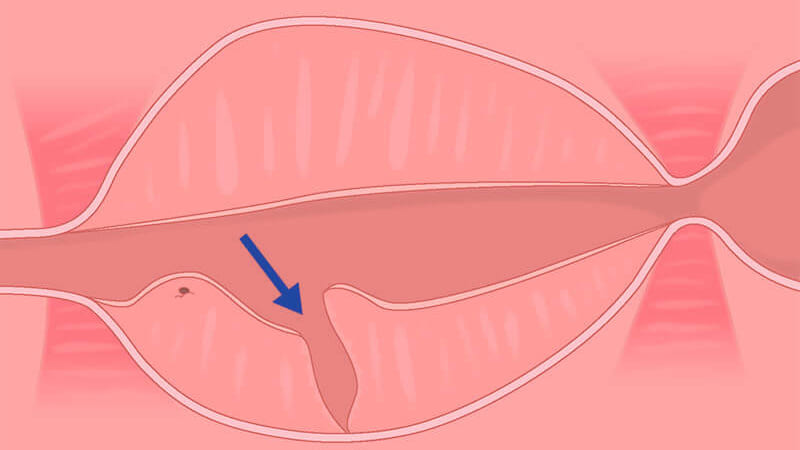
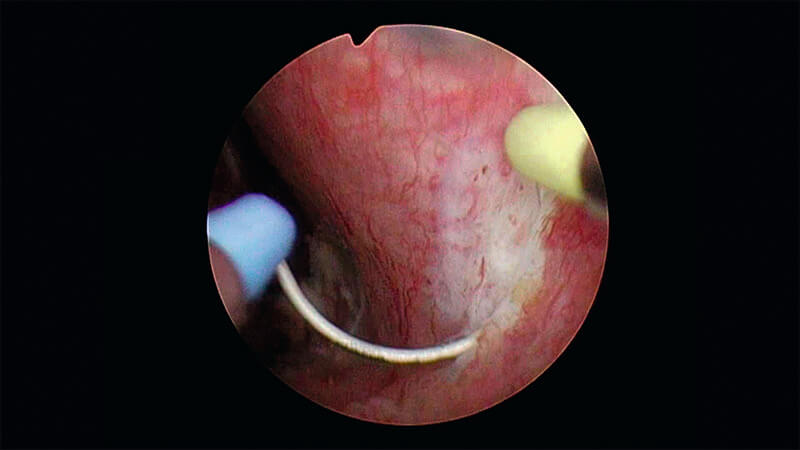
Perform a prograde incision distally and laterally of the verumontanum until the surgical prostate capsule is reached.
Cut approximately 1–2 loops deep until the surgical capsule is identified.
If ejaculatory function is to be spared the incision around the verumontanum should be at a distance of approx. 2 loop diameters.
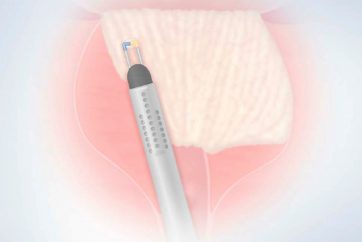
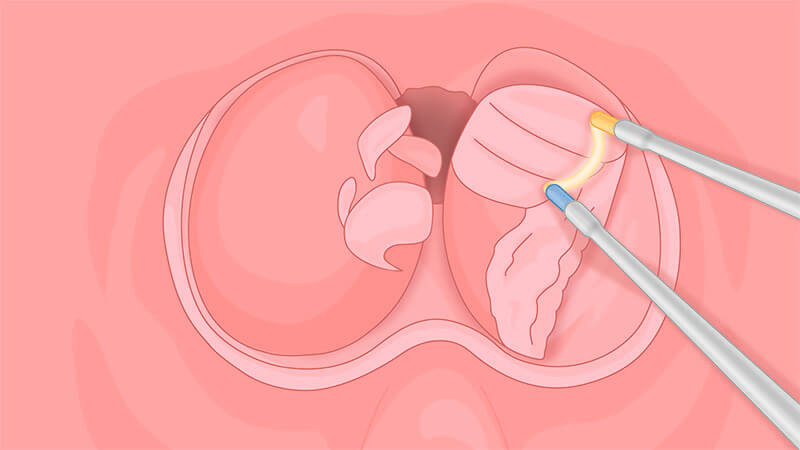
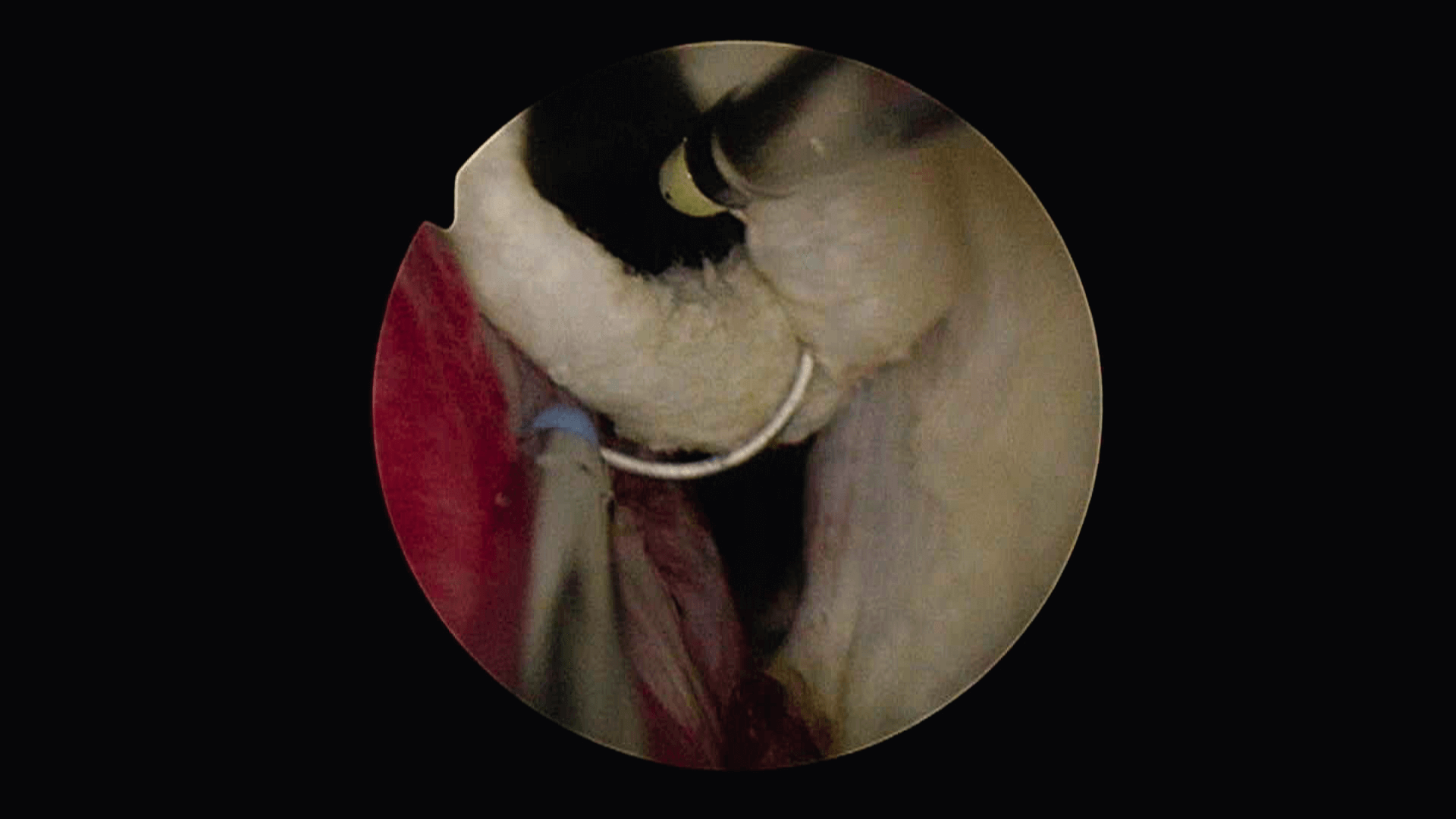
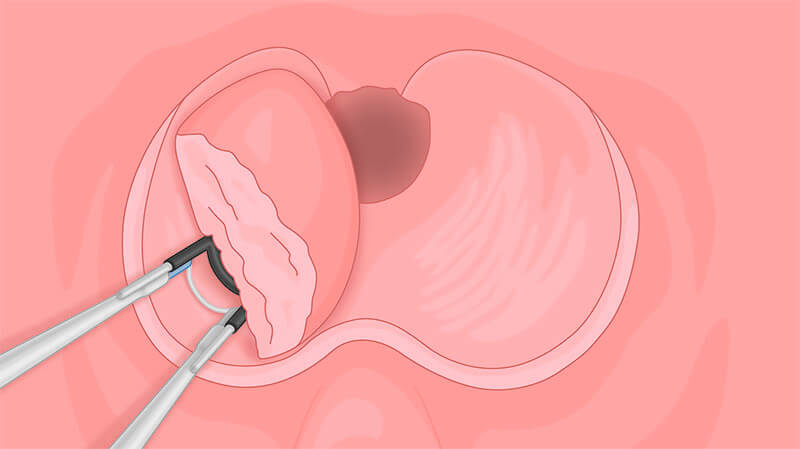
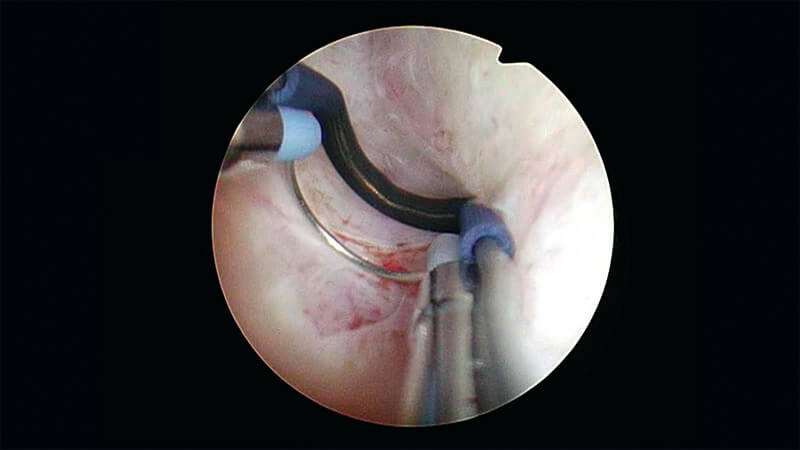
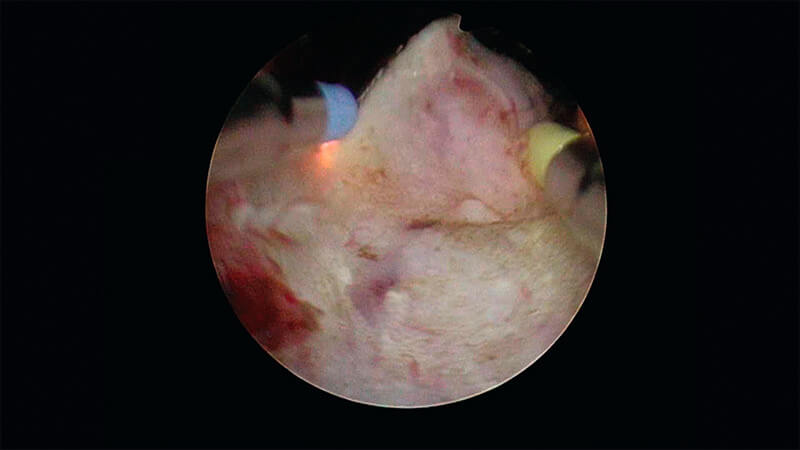
05 | Enucleation of Left Prostate Lobe
Mechanical Separation of the Left Prostate Lobe from the Capsule.
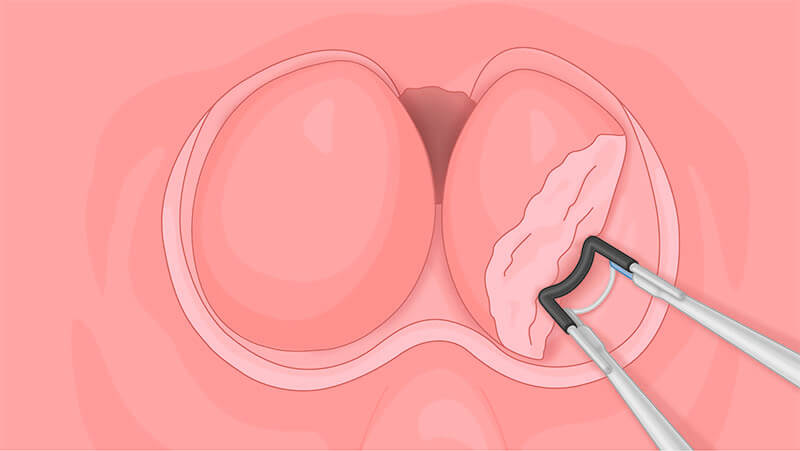
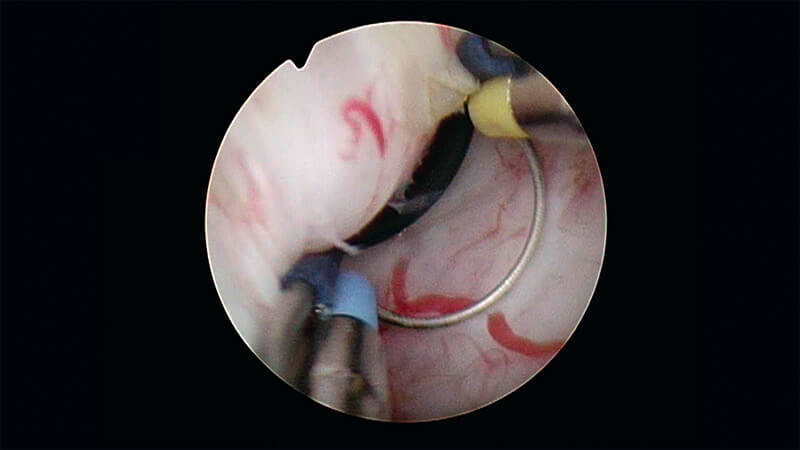
Find the plane between capsule and prostatic lobe and separate the adenoma from the capsule by using the spatula of the TUEB electrode as a lever.
Separate the tissue and the capsule step by step without too much force in one single push.
Leave a bridge of tissue at the bladder neck at the 5 o’clock position. In this way the enucleated lobe is held in position and can swiftly be resected. A free-floating prostate lobe is very difficult to dissect with a loop electrode. In this case a morcellator is helpful.
If bleeding occurs, use the loop for hemostasis. Put slight pressure on the bleeding without moving backwards and forwards with the loop (as known from monopolar surgery). The coagulation mode will stop any small bleeding.
In most cases vessels are in the 11 and 1 o’clock positions.
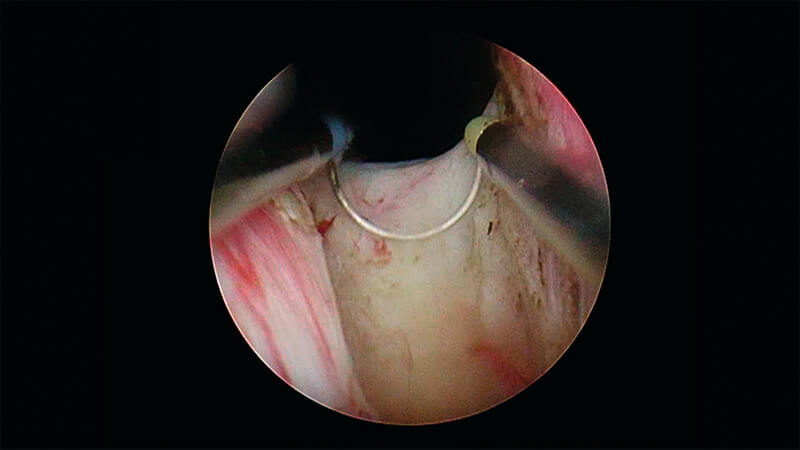
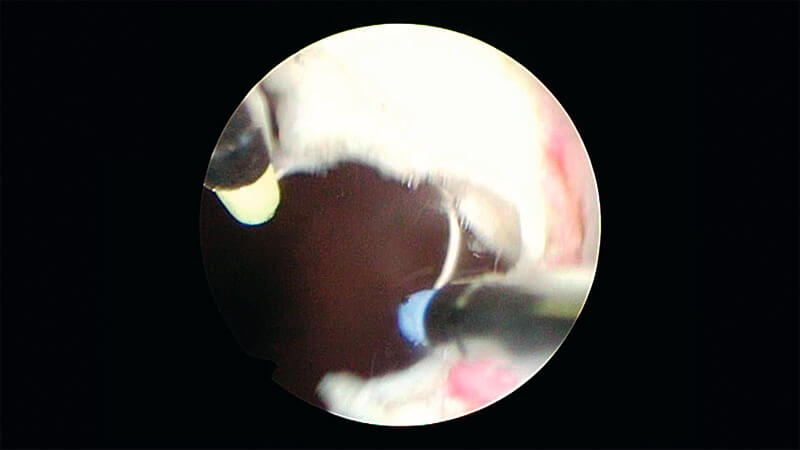
06 | Commissurotomy
Plasma Resection of the Prostate at the 12 O’Clock Position for Separation of the Lateral Lobes.
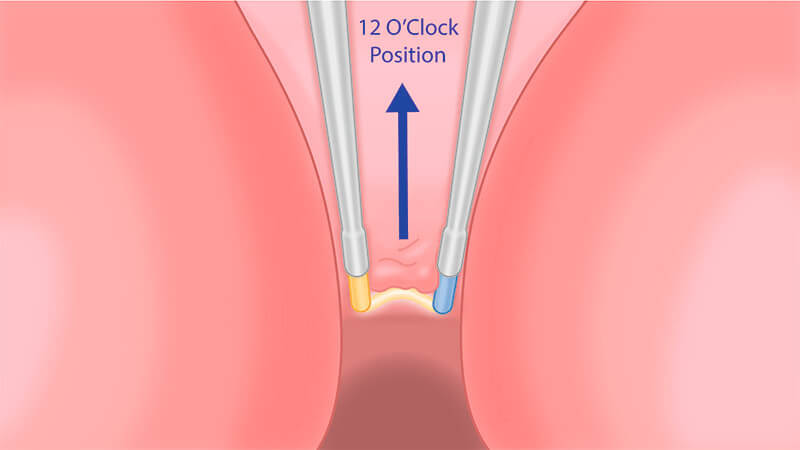
Change the TUEB electrode to regular TURis loop and start resecting.
Position tip of outer sheath on verumontanum to avoid unwanted cutting of sphincter.
07 | Resection of the Left Prostate Lobe
Plasma Resection of the Enucleated Lobe.
Resect the prostatic lobe layer by layer with the medium loop. There should be little or no bleeding.
After full resection of the adenoma, resect the tissue bridge without cutting into the prostatic capsule. Here regular bleeding can occur.
08 | Evacuation of Resected Tissue
Only If a Separated Histological Specimen Is to Be Evaluated.
09 | Initiation of Enucleation of the Right Prostate Lobe
Paracollicular Prograde Incision with Plasma of the Mucosa of the Right Lobe.
Perform a prograde incision distally and laterally of the verumontanum until the surgical prostate capsule is reached.
Cut approximately 1–2 loops deep until the surgical capsule is identified.
If ejaculatory function is to be spared the incision around the verumontanum should be at a distance of approx. 2 loop diameters.
10 | Enucleation of Right Prostate Lobe
Mechanical Separation of the Right Prostate Lobe from the Capsule.
Find the plane between capsule and prostatic lobe and separate the adenoma from the capsule by using the spatula of the TUEB electrode as a lever.
Separate the tissue and the capsule step by step without too much force in one single push.
Leave a bridge of tissue at the bladder neck at the 7 o’clock position. In this way the enucleated lobe is held in position and can swiftly be resected. A free-floating prostate lobe is very difficult to dissect with a loop electrode. In this case a morcellator is helpful.
If bleeding occurs, use the loop for hemostasis. Put slight pressure on the bleeding without moving backwards and
forwards with the loop (as known from monopolar surgery). The coagulation mode will stop any small bleeding.
In most cases vessels are in the 11 and 1 o’clock positions.
11 | Resection of Right Prostate Lobe
Plasma Resection of the Enucleated Lobe.

Resect the prostatic lobe layer by layer with the medium loop. There should be little or no bleeding.
After full resection of the adenoma, resect the tissue bridge without cutting into the prostatic capsule. Here regular bleeding can occur.
12 | Resection of Apex
Plasma Resection of Apical Part of the Prostate to Ensure Best Flow Conditions.
Resect any residual adenoma at the apex of the prostate.
Make sure not to cut into the sphincter to prevent incontinence after the intervention.
13 | Trimming of the Bladder Neck and Hemostasis
Plasma Resection of the Bladder Neck to Ensure Best Flow Conditions.
Resect any residual adenoma at the bladder neck.
Evacuate prostate chips with a bladder syringe.
Ensure secure hemostasis.
Ensure warm saline is used (37°).
Be aware of bleeding and do spot coagulation where needed. Place the loop with slight pressure on the bleeding, activate coagulation mode and hold until bleeding has stopped.
- Content Type