Mechanical Lithotripter
Shomei’s Strategy – LithoCrushV™ Mechanical Lithotripter

Shomei Ryozawa, MD
Professor and Chairman, Department of Gastroenterology,
Saitama Medical University International Medical Center
Dr. Shomei Ryozawa, MD, the authoring Physician of this document, is a paid consultant of the Olympus Corporation, its subsidiaries and/or its affiliates.
Any content or information presented herein is illustrative in nature and does not guarantee or represent specific information, outcomes, or results. Under no circumstances shall Olympus or its employees, consultants, agents, or representatives be liable for any Under no circumstances shall the Olympus Group or its employees, consultants, agents or representatives be liable for costs, expenses, losses, claims, liabilities or other damages (whether direct, indirect, special, incidental, consequential or otherwise) that may arise from or be incurred in connection with this information or any use thereof.
Any claims and/or comparisons within this article are solely the opinion of Dr. Shomei Ryozawa, MD. Olympus Corporation of America’s and its parents, subsidiaries, affiliates, directors, officers, employees, agents, and representatives (collectively Olympus) do not represent to or warrant the accuracy, reliability, or applicability of the Content.
Minimize Incision
EST is always the first choice. We keep the incision area for EST at the requisite minimum level (high frequency setting: ESG-100 pulse cut slow 30 W). We apply EPBD when EST appears too risky – for example, patients with coagulopathies, patients taking oral antithrombotic drugs, patients with an extremely small papilla, patients with periampullary diverticulum and patients with surgically altered anatomy.
In general, however, EST is indicated for almost all cases. EPLBD is indicated for large and multiple stones with bile duct dilatation that are difficult to treat by EST and EPBD alone. We normally perform EST before EPLBD. The precut technique are used after conventional methods of biliary cannulation and the pancreatic guidewire-assisted technique have failed.
Device Selection Criterion
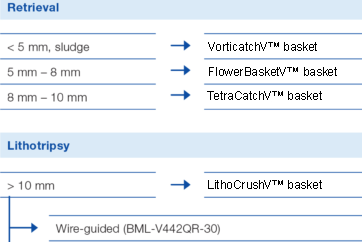
The basket is our preferred choice when dealing with stones. We use VorticCatchV™ basket for small stones under 5 mm and sludge, the 8-wire FlowerBasketV™ basket for stones from 5 to 8 mm, the 4-wire TetraCatchV™ basket for stones from 8 to 10 mm, and the lithotripsy basket (LithoCrushV™ basket) for stones over 10 mm.
In situations where the basket catheter has difficulty grasping the stones – with small stones, intrahepatic stones, or a pocket-shaped distal bile duct, for example – we use the retrieval balloon.
Cases Where Lithotripsy has Been Used
The best way to perform EPLBD is to dilate the duct at low pressure. This helps to minimize the load on, and the risk to, the duodenal papilla and bile duct. In our opinion, the low-pressure setting of the StoneMasterV™ device is best suited for this purpose.
When using StoneMasterV™ device previously, we have always found dilation to be more than adequate and have never experienced any problems when performing a procedure. We also believe that low-pressure dilation even with a large-size 18 mm-diameter balloon can support safer EPLBD procedures.
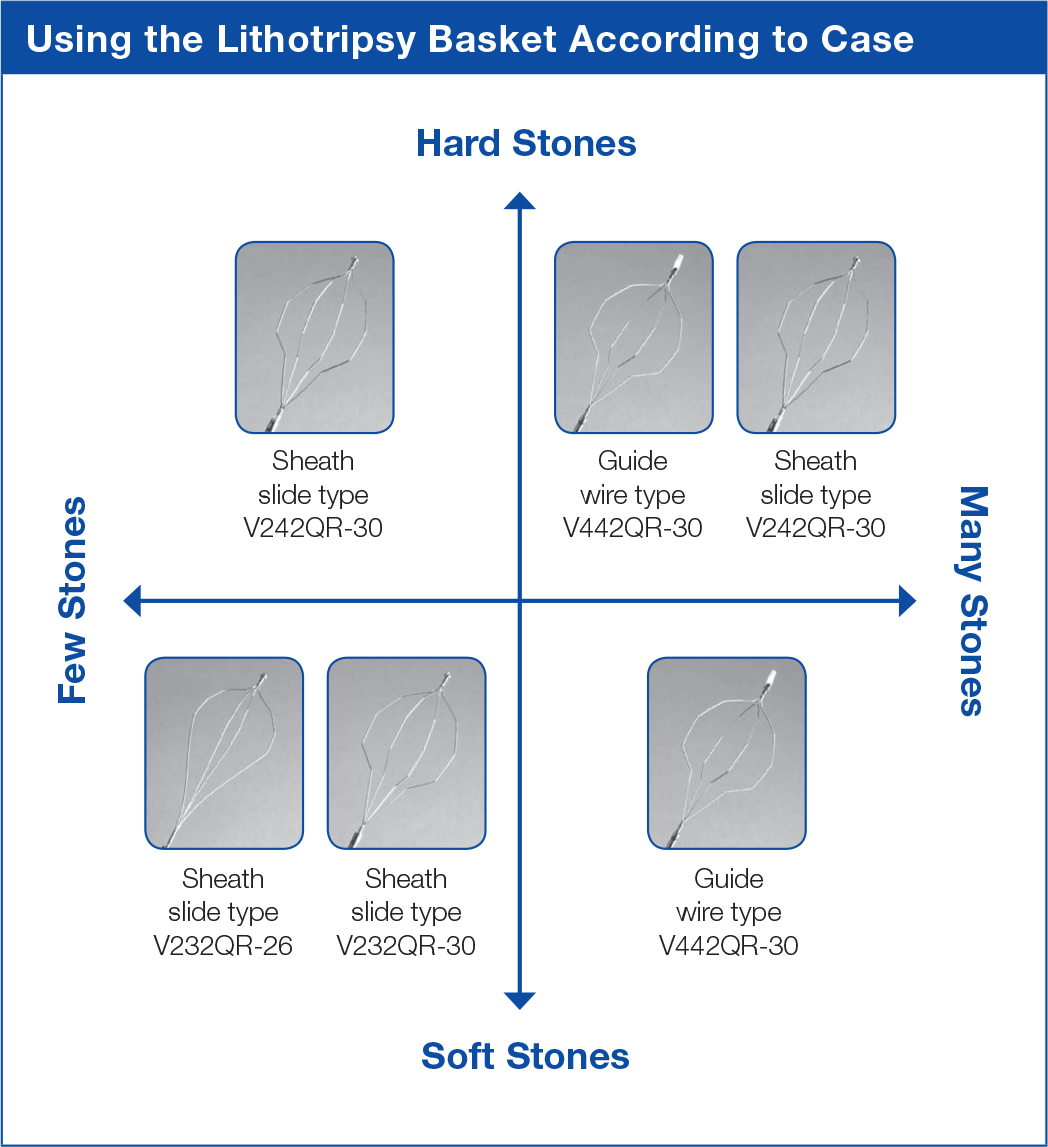
Using the LithoCrushV™ Basket
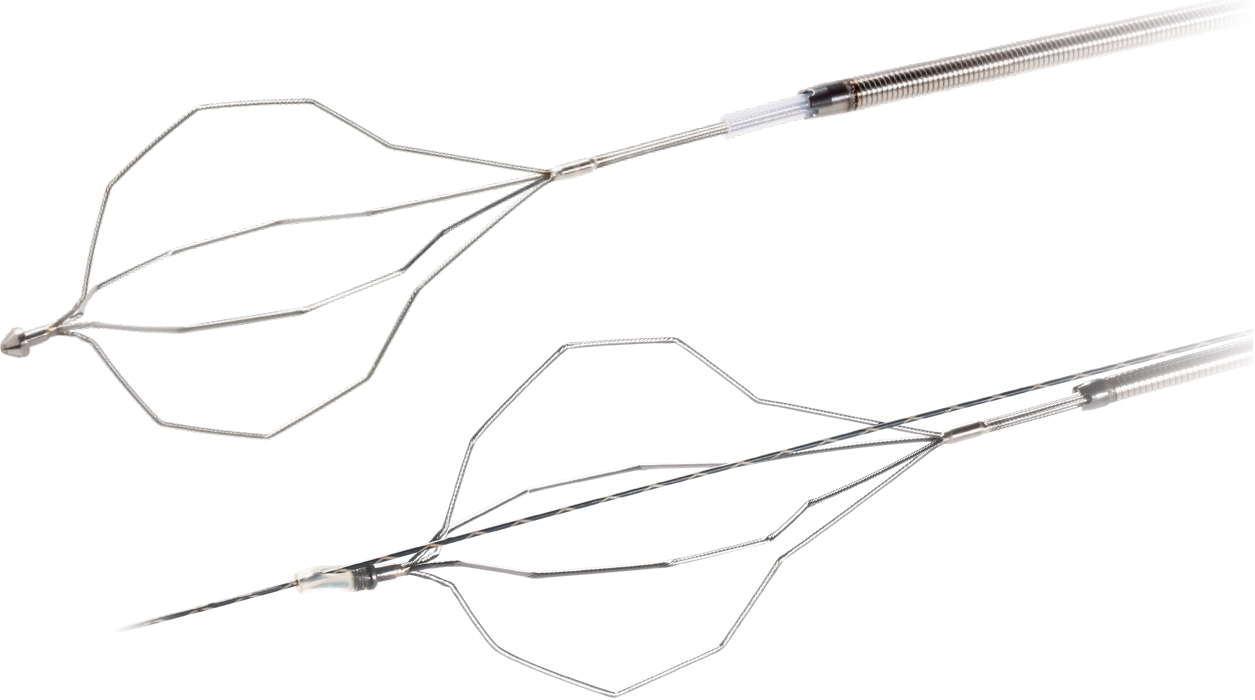
The first choice is the wire-guided type (BML-V442QR-30), which is the easiest to use and offers excellent access. Before introduction of the wire-guided type, it was very difficult to guide the retrieval basket to the bile duct. While the guidewire and basket are installed in parallel on some wire-guided models, they are coaxial on the LithoCrushV™ basket, which makes insertion remarkably easy.
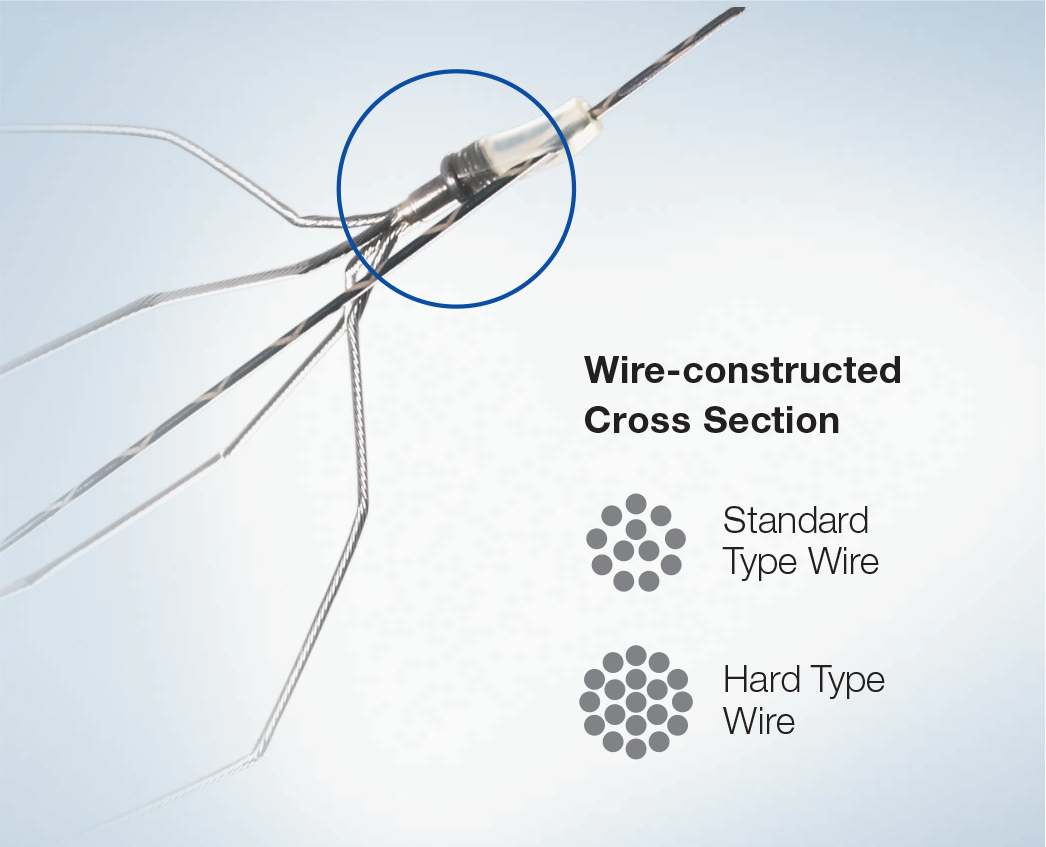
In cases where CT imaging shows that the stone may be difficult to grasp, we use the hard-wire type (BML-V242QR-30), which has more coils than the standard type.
Because the extra coils provide excellent expansion force, switching to the hard-wire type may make retrieval possible in cases where it is difficult to grasp the stones during a procedure.
The LithoCrush line also includes two standard wire type models with a sheath slide mechanism.
Stone Retrieval Technique
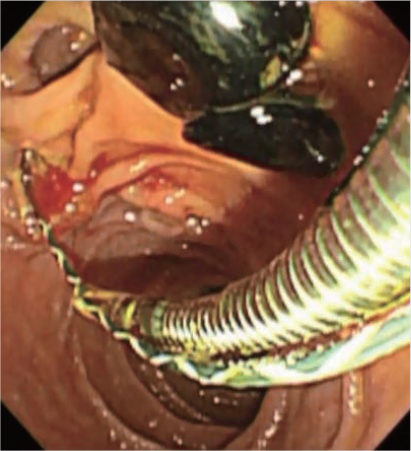
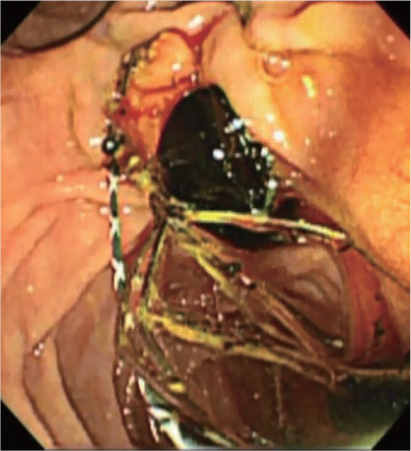
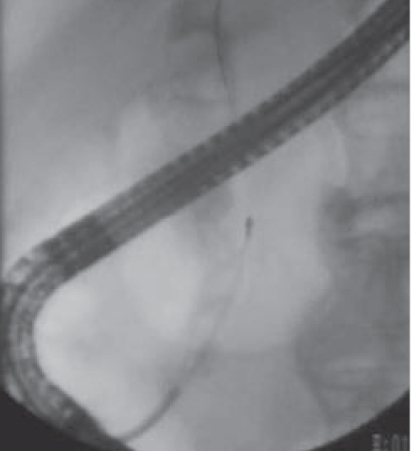
The standard retrieval technique is to expand the basket above the stones, then shaking the basket a little at a time to grasp the stones (see endoscopic and radiological images below).
The LithoCrushV™ basket also incorporates a “basket rotation function”, which can be used when the standard method does not appear to be working. Even during use of the wire-guided type, the rotation facility can be used by withdrawing the guidewire.
Occasionally, it may be difficult to grasp stones in the hilar area or the hepatic or intrahepatic bile ducts. In this case, withdrawing the guidewire before approach may facilitate extraction.
BML-V442QR-30 (Wire-guided hard type)
Preventing Basket Deformation
Many doctors believe that it is not necessary to close (tighten) the basket fully. We share that belief. If the stones have been crushed before the basket has fully closed, there is no reason to tighten the basket any further. This also seems to help prevent deformation of the basket (see diagram below).
Olympus is a registered trademark of Olympus Corporation, Olympus America., Incorporated and/or their affiliates
- Content Type




