GENERAL INFORMATION ABOUT THYROIDECTOMY
Indications for Thyroidectomy
One of the major indications is a diagnosis of thyroid cancer.
Also, the existence of cold or hot thyroid nodules could be an indication for operative treatment.
Besides malignancies, thyroidectomy is also an option for patients with symptomatic thyroid masses or goiters. The patients have compressive symptoms including dysphagia, dyspnea, shortness of breath, and/or hoarseness due to a large goiter.
Cosmetic concerns due to an enlarged but symptom-free goiter may also be an indication for thyroidectomy.
Another indication would be with medically refractory autoimmune diseases (like Grave’s disease) or hyperthyroidism.
Types of Thyroidectomy
Depending on the indication, a thyroidectomy can include total or partial removal of the gland. For malignant diseases, the total removal of the gland is recommended.
In the case of benign pathologies that do not affect the entire thyroid gland, a lobectomy with or without isthmusectomy is sufficient.
Surgical Treatment Options
Thyroid surgery can be performed with conventional or minimally invasive techniques.
Conventional open thyroidectomy is still a standard procedure that includes a collar incision of a few centimeters depending on the indication.
For thyroid tumors smaller than 3 cm, a minimally invasive technique could be an option. The approach to the thyroid gland can be cervical (MIVAT = minimally invasive video-assisted thyroidectomy) or extracervical (axillary approach, chest approach, or clavicular approach).
Special imaging equipment and instruments are needed.
Challenges in Thyroid Surgery
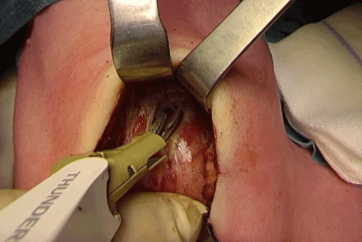
A total or partial thyroidectomy can be a challenging procedure due to the complex anatomy of the gland, the limited space in the cervical area, and the surrounding structures such as nerves (e.g. recurrent laryngeal nerve) blood vessels, and several muscle layers. There is a risk of damaging these sensitive structures during surgery causing intra- and postoperative bleeding or vocal-nerve damage.
In particular, damage to the recurrent laryngeal nerve can result in paralysis of the vocal cords.
Anatomical variations of the thyroid gland and how it is attached to the surrounding tissue due to the disease could also present challenges during surgery.
Surgical Equipment
General
- Suction/irrigation unit
- ESG-400 high-frequency generator (monopolar pencil, often bipolar forceps)
- USG-400 ultrasound generator
- THUNDERBEAT
- Neuromonitoring generator for IONM
- Tracheotomy set
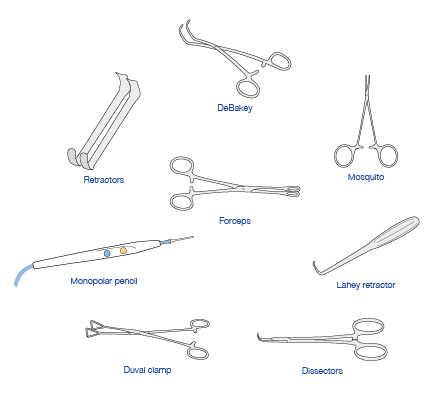
Instruments for Open Surgery
- Scalpel
- Tweezers
- Scissors
- Needle holder
- Clamps
- Forceps
Further OR Equipment:
- Ligating clip appliers
- Suture: 3-0 and 4-0 for ligation and for subcutaneous wound closure
- Drainage
- Drapes

GENERAL INFORMATION ABOUT THYROIDECTOMY
Intraoperative Neuromonitoring IONM
The intraoperative identification and monitoring of the vocal nerves (vagus nerve, superior/inferior/recurrent laryngeal nerves) in order to protect them during surgery is mandatory.
Any nerve injury or malfunction due to intraoperative compression, crushing, thermal injury, ischemia, ligature, stretching, or traction has to be prevented.
Intermittent stimulation of the dissected field allows tracing of the nerve and its branches differentiating nerve from nearby non-nervous tissue.
The nerves’ vitality and intraoperative prediction of postoperative vocal cord function are constantly checked with a stimulation electrode to detect any visible or audible signal changes immediately. The electrode signals are also documented.
Identification of the Vocal Nerves
Identification of the vocal nerves (vagus nerve, superior/inferior/recurrent laryngeal nerves) during surgery for safe dissection, constant checking of nerve vitality, and intraoperative prediction of postoperative vocal cord function, including intraoperative documentation of nerve activity.
A stimulation electrode with 0.5–1 mA is placed on the nerves.
A generator is monitoring nerve activity and enables the surgeon to detect any visible / audible signal changes immediately.
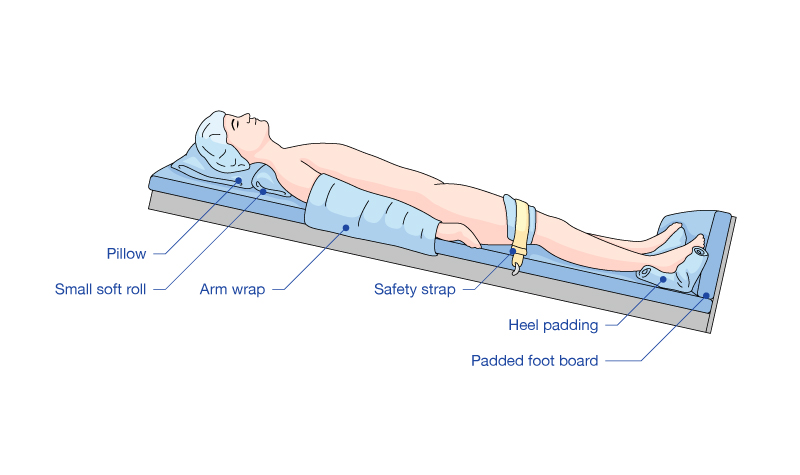
PATIENT PREPARATION AND POSITION OF SURGICAL TEAM
The patient is placed on the operation table in a supine position. A pillow is placed under the patient’s shoulder because the neck needs to be slighty hyperextended. The table is tilted in a 20° anti-Trendelenburg position.
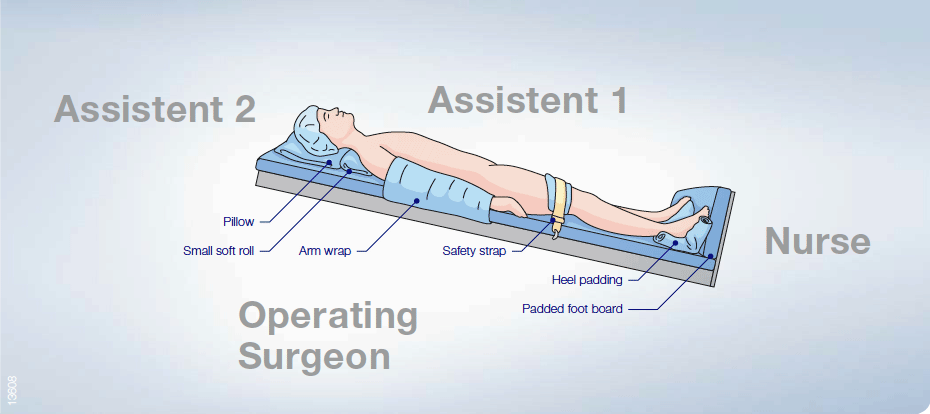
The surgeon stands on the right or left side, contralaterally to the side of operation. In this brochure, the described thyroidectomy is started on the left side. Thus the surgeon is located at the patient’s right side. Assistant 1 is on the opposite side of the surgeon and assistant 2 is positioned toward the patient’s head. The nurse is positioned at the patient’s feet. During a total thyroidectomy, the surgeon and the assistant 1 change sides.
- Keyword
- Content Type