Inspect Oral Cavity Patterns Disclaimer
NBI is crucial in the early diagnosis of oral cavity cancer. A deep knowledge of NBI patterns in the different oral subsites could help in differentiating normal epithelium from dysplastic and neoplastic lesions.

Francesca Boscolo Nata, MD
ENT Clinic, Head and Neck Department University of Trieste, Italy

Giancarlo Tirelli, MD
ENT Clinic, Head and Neck Department University of Trieste, Italy
The following pictures highlight the main characteristics of oral cavity NBI patterns in the different epithelial types.
· Normal pattern is different in each epithelial type.
· Dysplastic pattern is similar in epithelial types 1 and 2a, and different in type 2b.
· Neoplastic pattern is similar in all the epithelial types. Vessels are visible in vegetating areas of the lesion, while they are absent in ulcerated areas because of the presence of necrotic tissue.
Anatomy and Mucosal Structure in Oral Cavity
We can identify three different mucosal structures in oral cavity (Lin et al., 2012):
Type 1 (yellow)
Keratinized thick stratified squamous epithelium in gingiva, hard palate and dorsal surface of the tongue.
Type 2a (green)
Nonkeratinized thin stratified squamous epithelium in the floor of the mouth and ventral tongue.
Type 2b (blue)
Nonkeratinized very thick stratified squamous epithelium in the retromolar trigone, labial and buccal mucosa.

Type 1 Epithelium
Normal Pattern
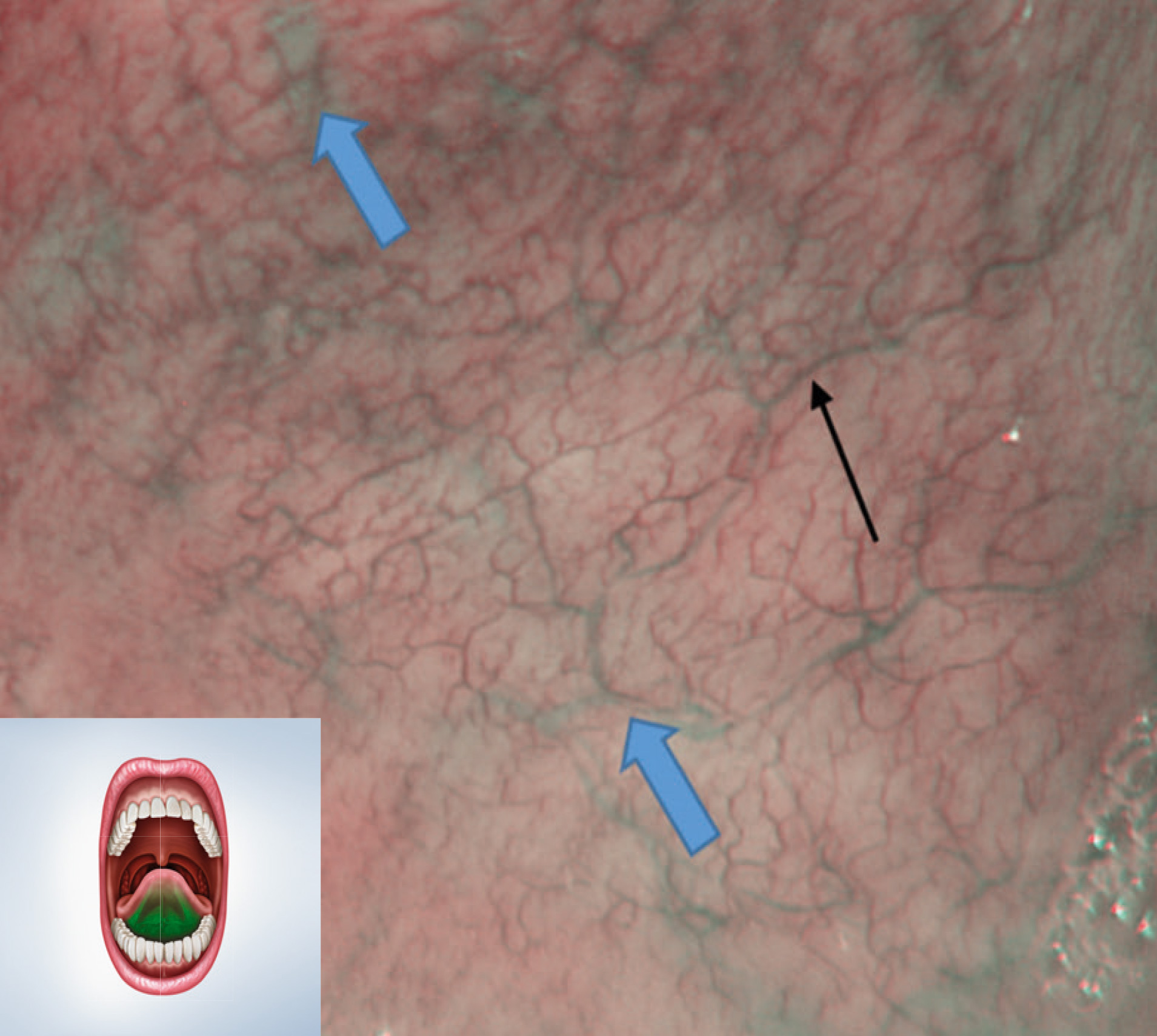
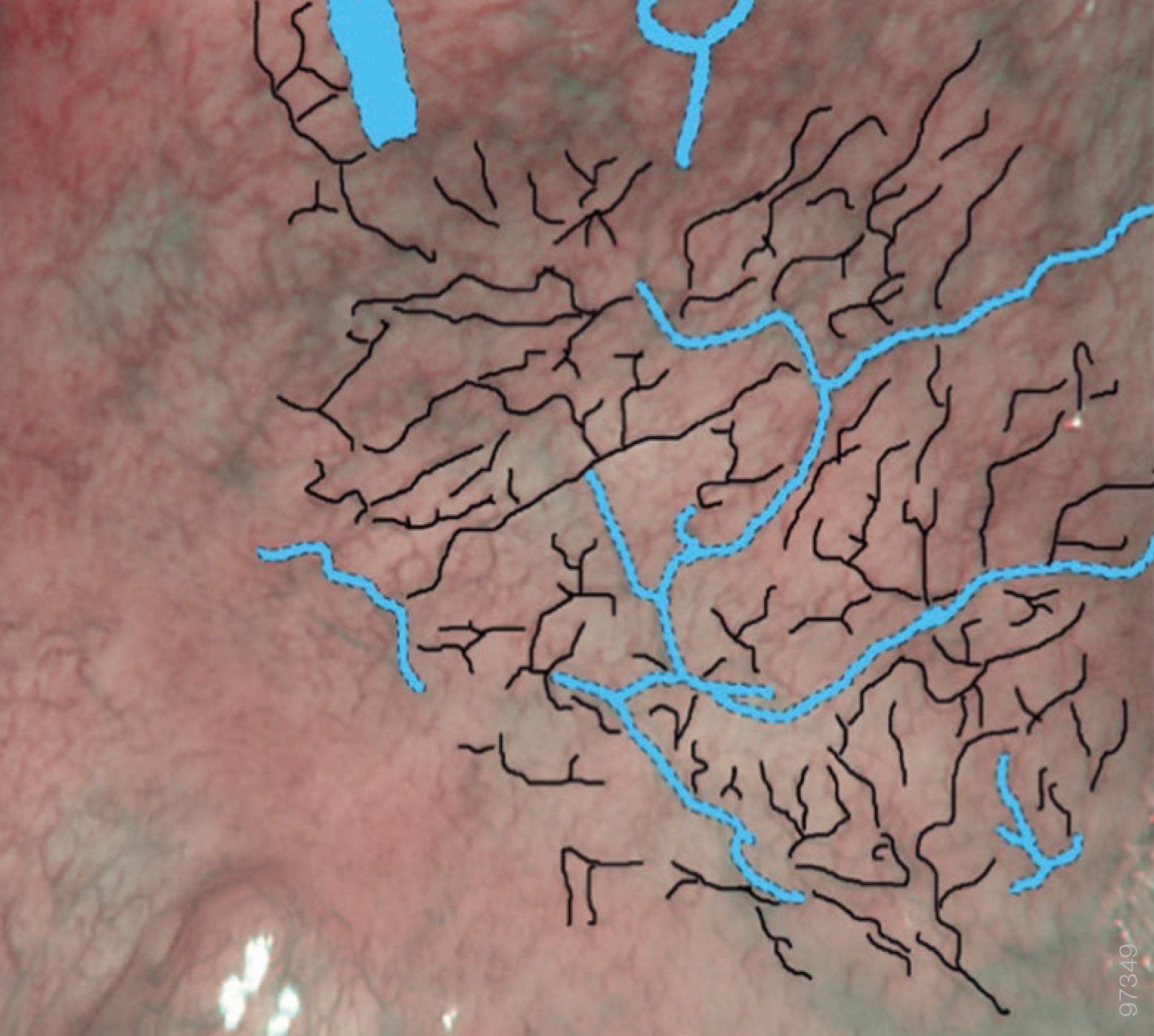
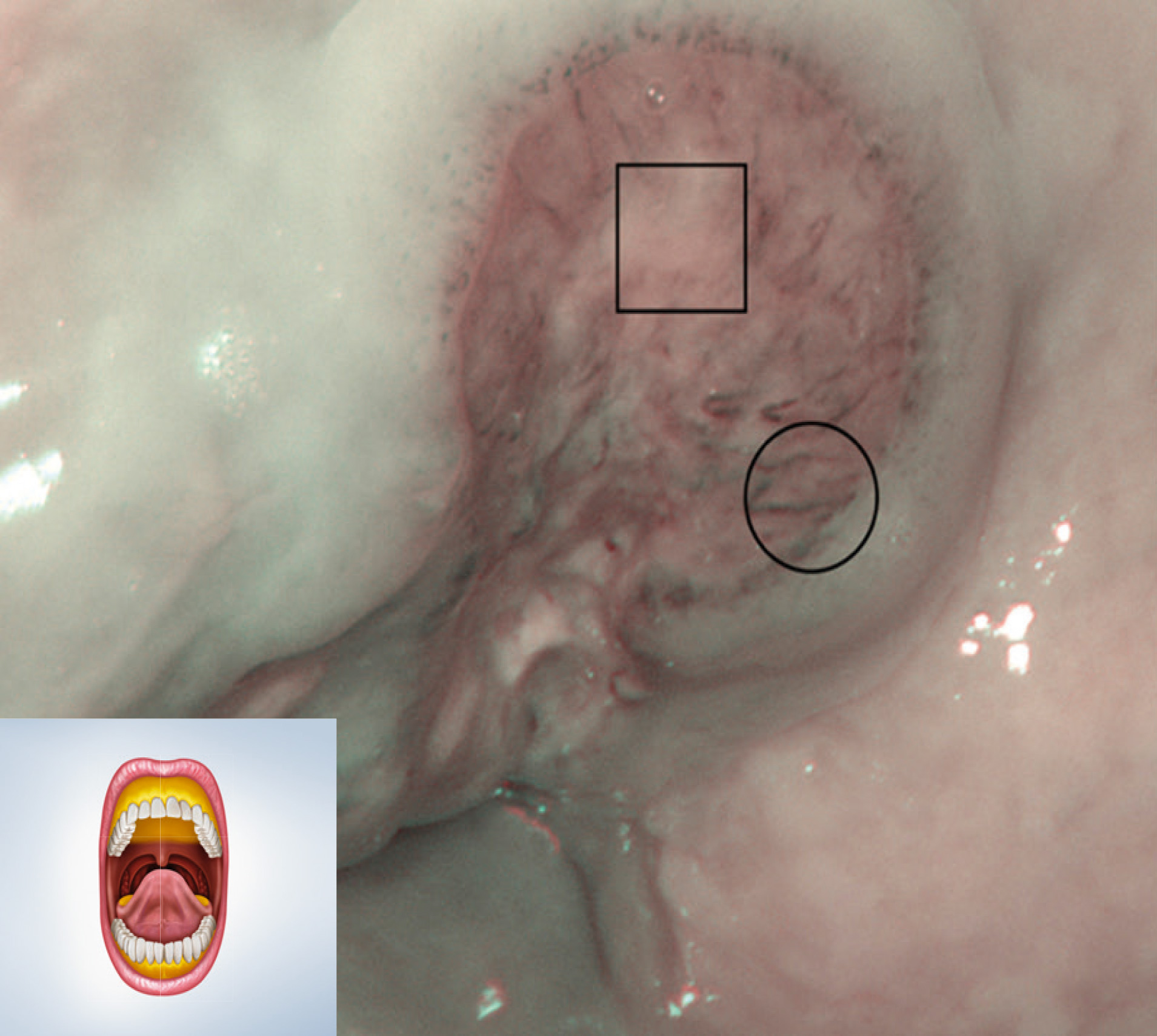
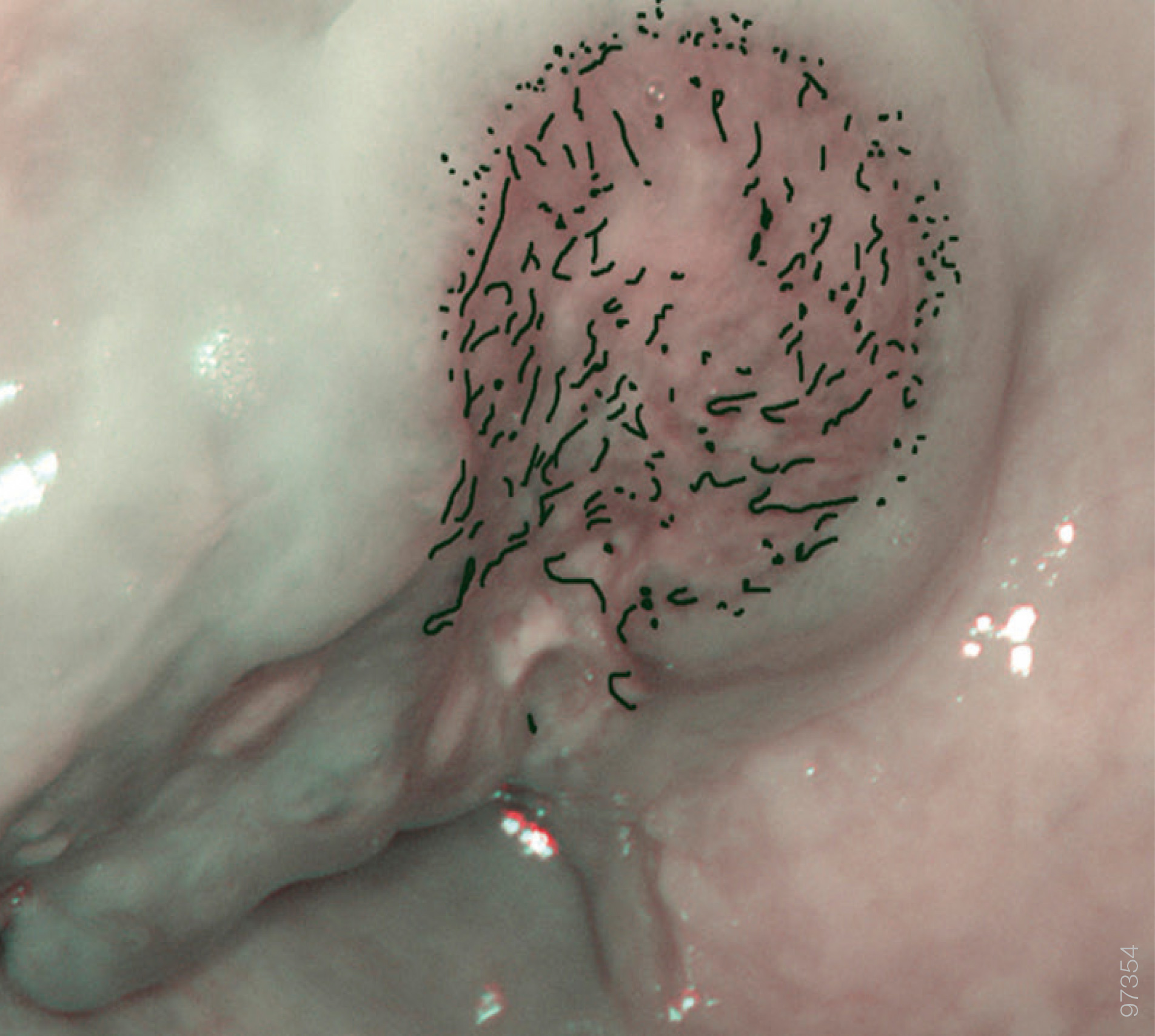
Gingiva, hard palate and dorsal surface of the tongue, normal pattern.


Posterior hard palate. Superficial mucosal capillaries appear as thin dark-green/brown vessels with small branches arising at an acute angle (thin black arrow). We can notice some “flower-like” configuration with a thin vessel acting as a “stem” and some points all around as the “petals” (〇), attributable to minor salivary glands. Some large light-blue vessels representing the submucosal veins can be glimpsed (thick light-blue arrow).
Type 2a Epithelium
Normal Pattern
Floor of the mouth and ventral tongue, normal pattern.
Floor of the mouth. Superficial mucosal capillaries appear as thin dark-green/brown vessels with small branches arising at an acute angle (black thin arrow). Submucosal veins are clearly visible as larger light-blue vessels (thick light-blue arrows).
Type 2b Epithelium
Normal Pattern
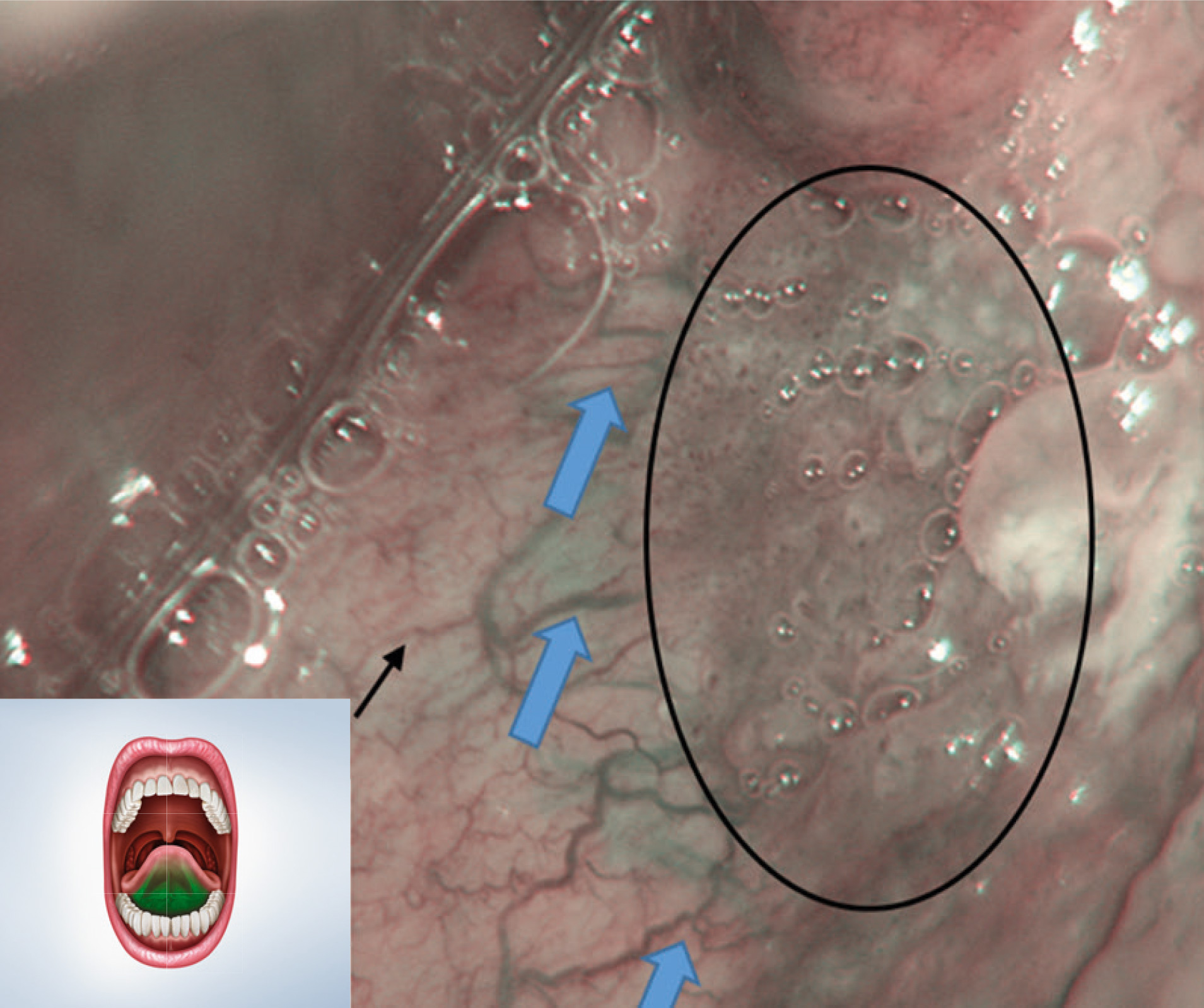
Retromolar trigone, labial and buccal mucosa, normal pattern.
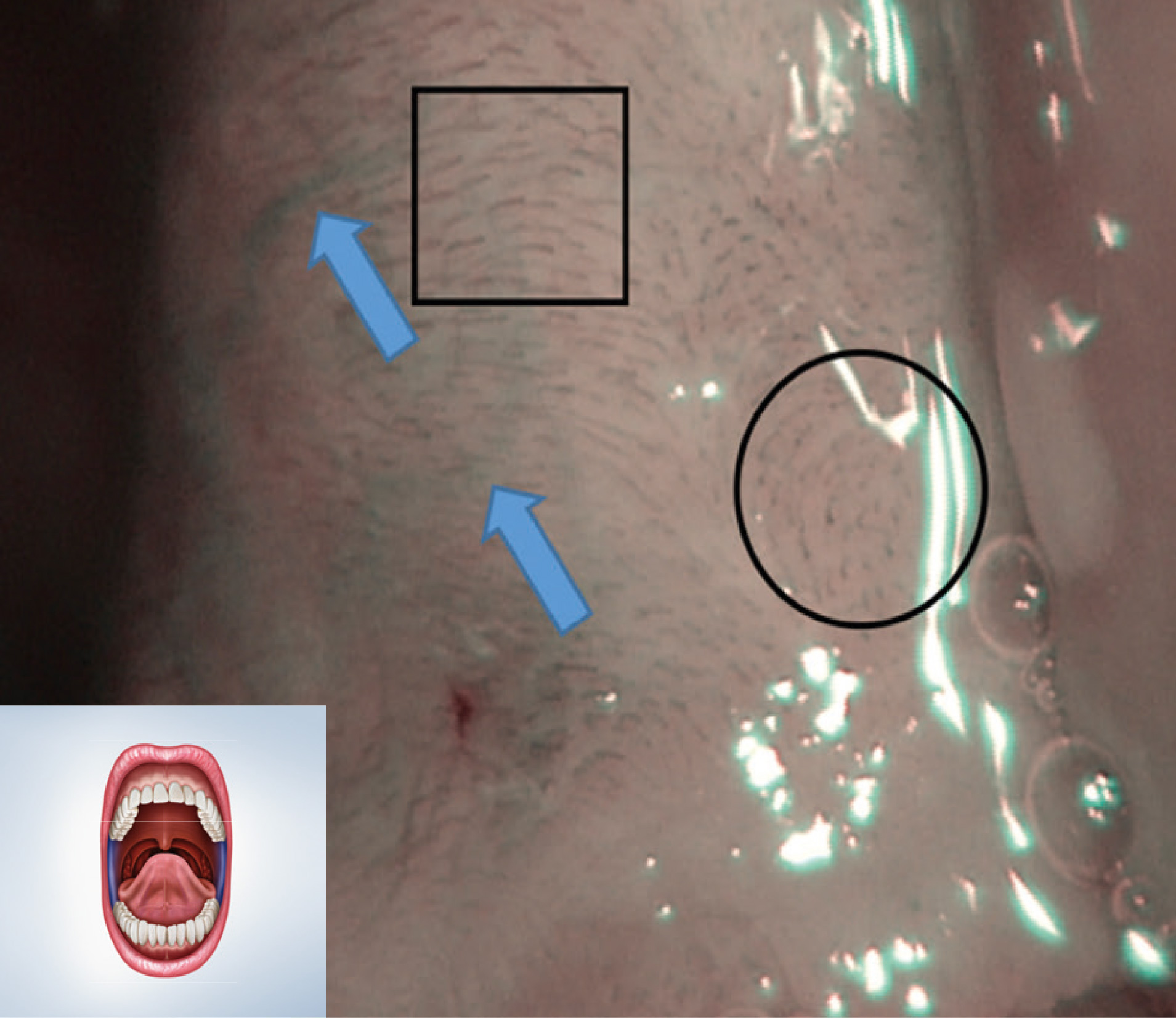
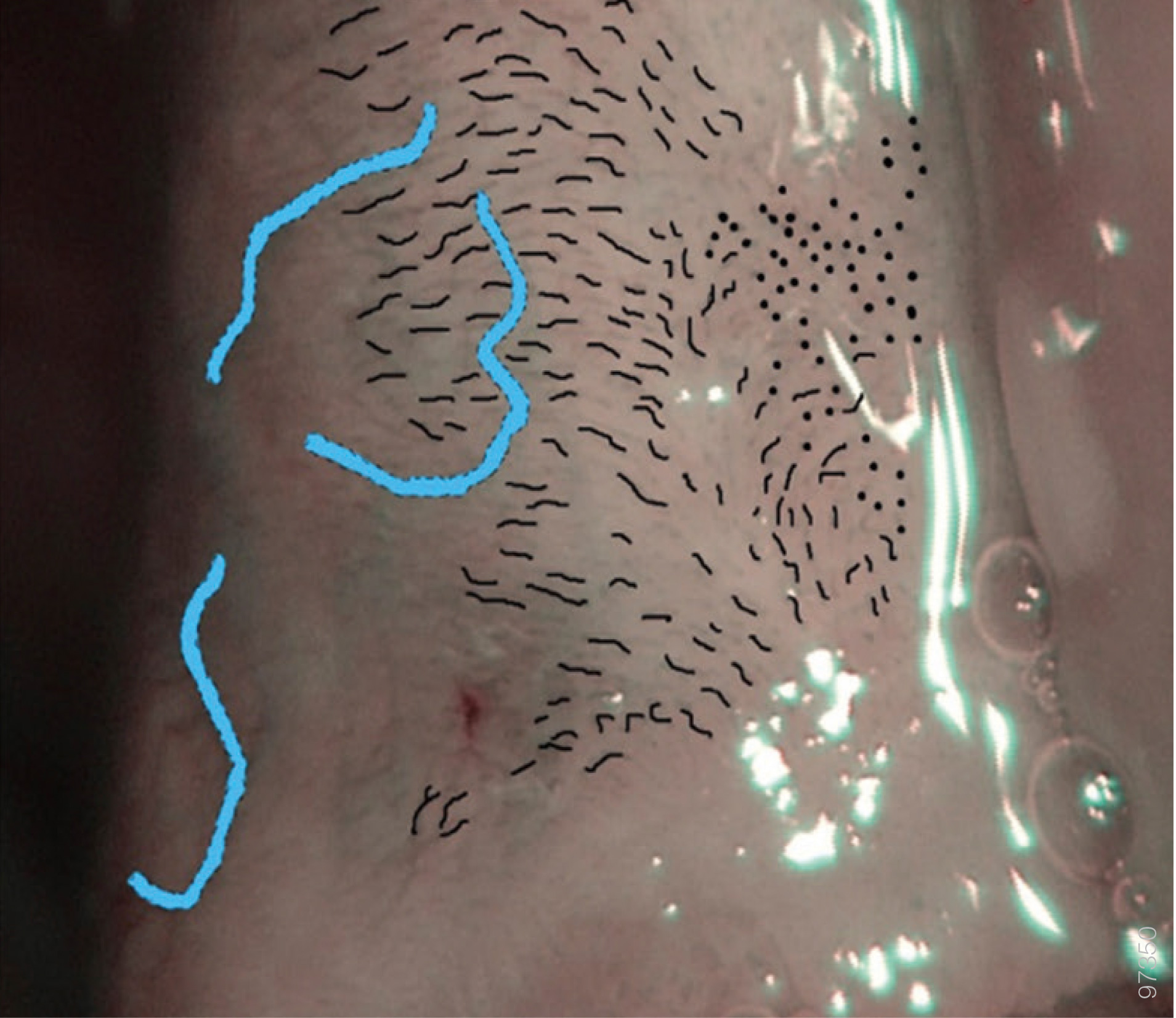
Left inferior trigone. Superficial mucosal capillaries appear as regular and equidistant dark-green/brown small punctuations (〇) if the vessels are visualized perpendicularly, or as short dashes (▢) if they are longitudinal to the mucosa. Submucosal veins can be glimpsed as some large light-blue vessels (thick light-blue arrows).
Type 1 Epithelium
Dysplastic Pattern
Gingiva, hard palate and dorsal surface of the tongue, dysplastic pattern.

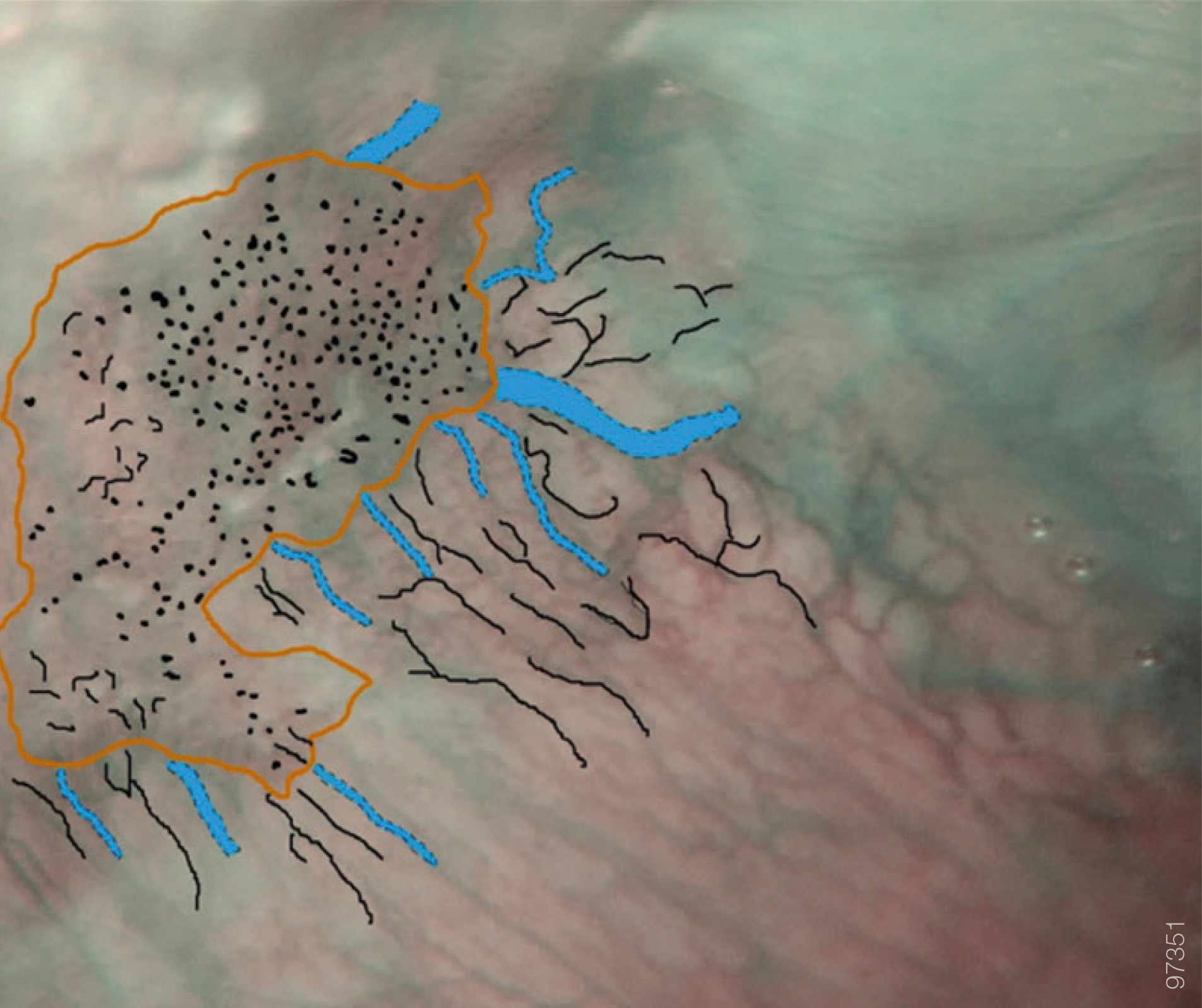
Posterior hard palate. The area with high-grade dysplasia is visible as a well-demarcated area with thick dark spots (〇); dilated light-blue vessels (thick light-blue arrows) reach this area perpendicularly. In the dysplastic area the submucosal large light-blue vessels are no longer visible. Superficial mucosal capillaries are still visible outside the dysplastic area as thin dark-green/brown vessels with small branches arising at an acute angle (black thin arrow).
Type 2a Epithelium
Dysplastic Pattern
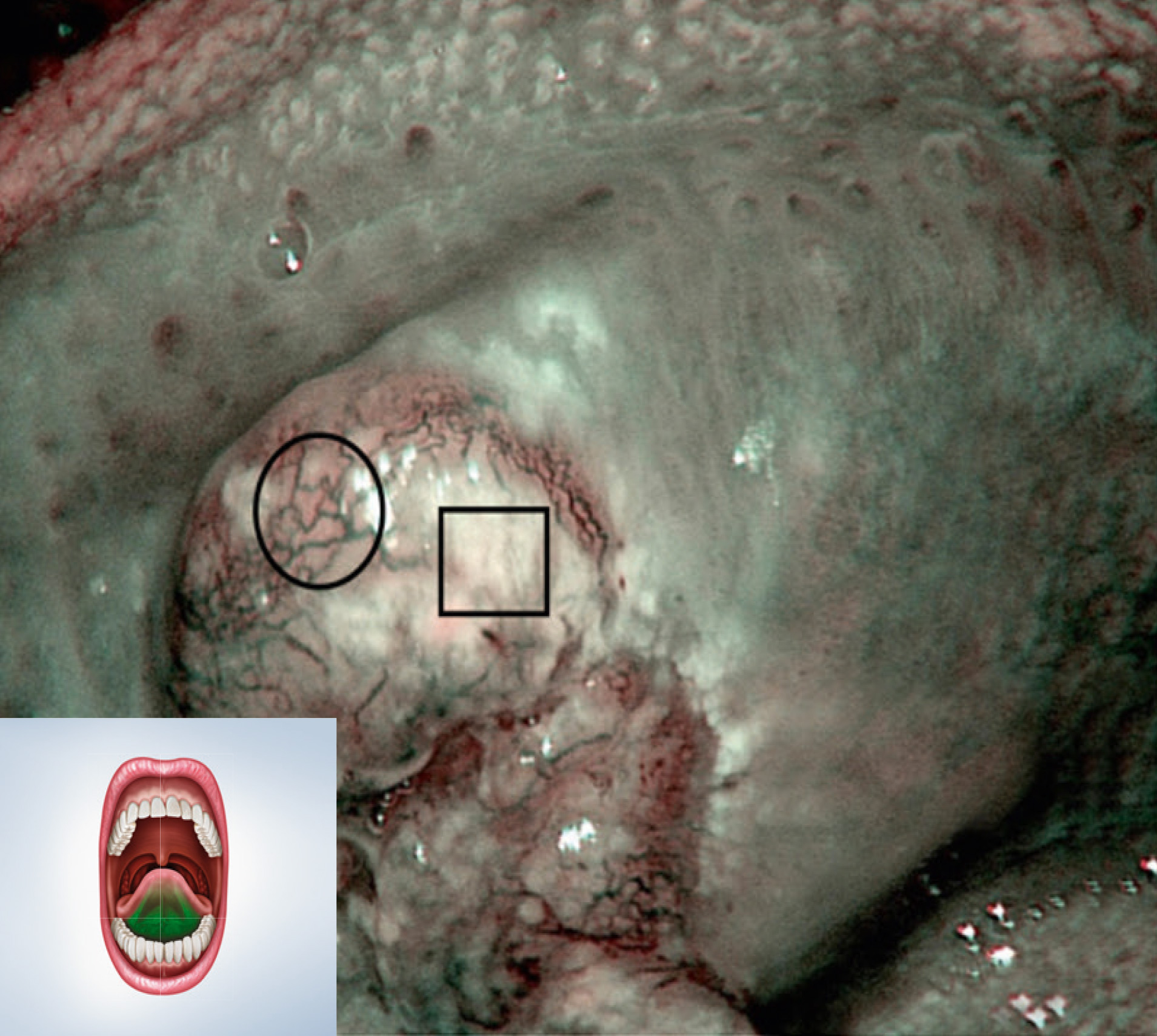
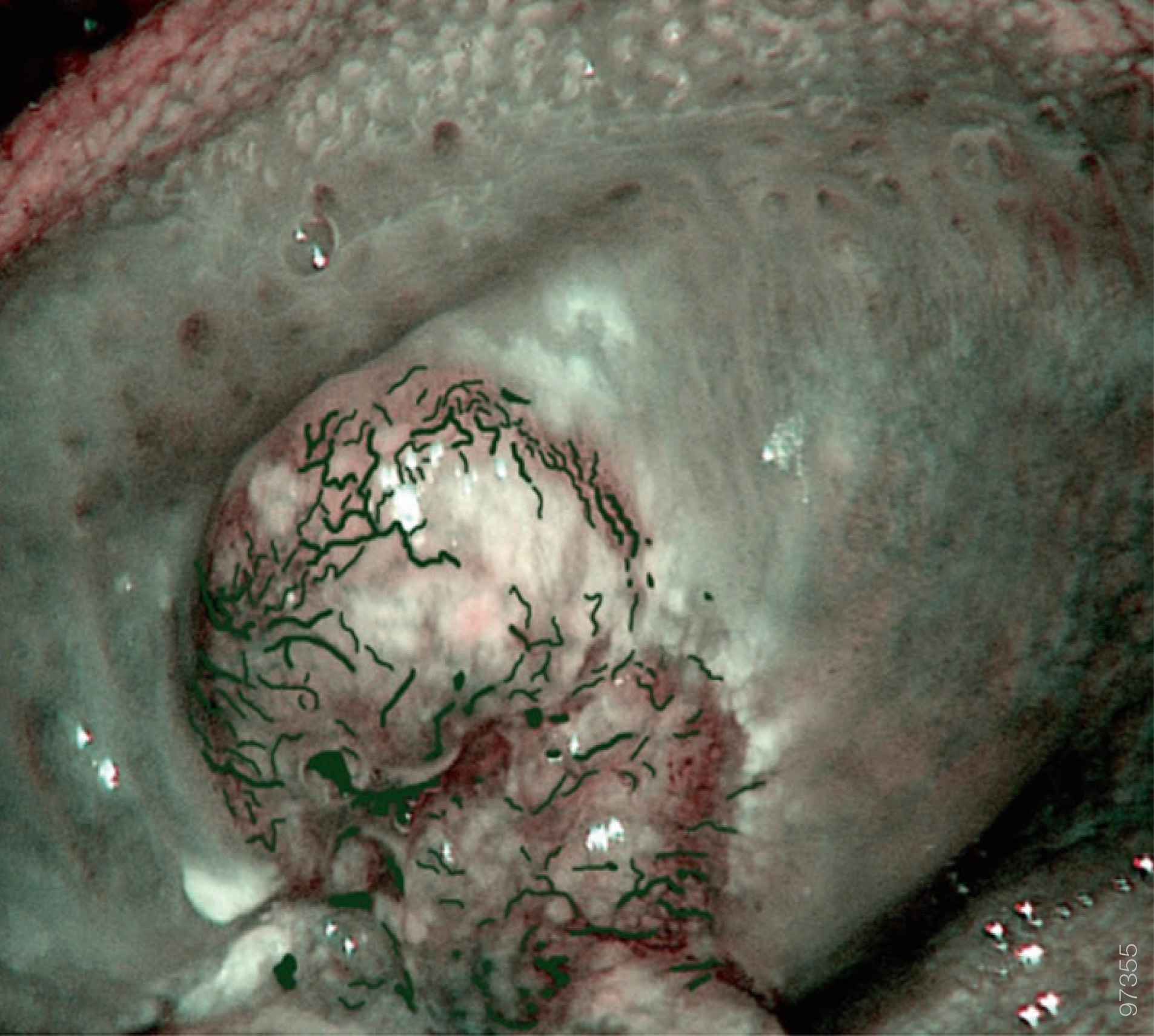
Floor of the mouth and ventral tongue, dysplastic pattern.
Floor of the mouth. The area with high-grade dysplasia is visible as a well-demarcated area with thick dark spots (〇); dilated lightblue vessels (thick light-blue arrows) reach this area perpendicularly. In the dysplastic area the submucosal large light-blue vessels are no longer visible. Superficial mucosal capillaries are still visible outside the dysplastic area as thin dark-green/brown vessels with small branches arising at an acute angle (black thin arrow).
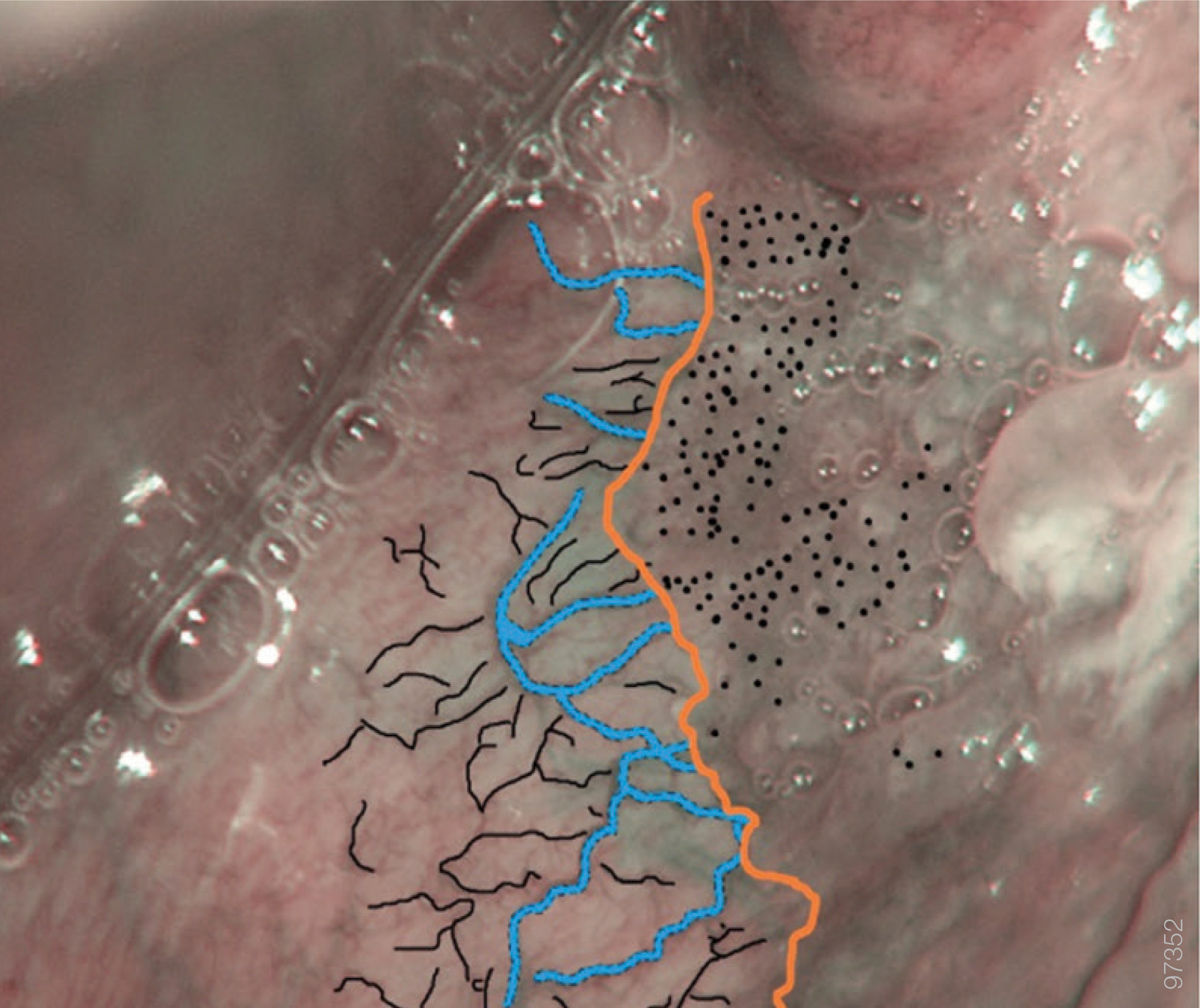
Type 2b Epithelium
Dysplastic Pattern
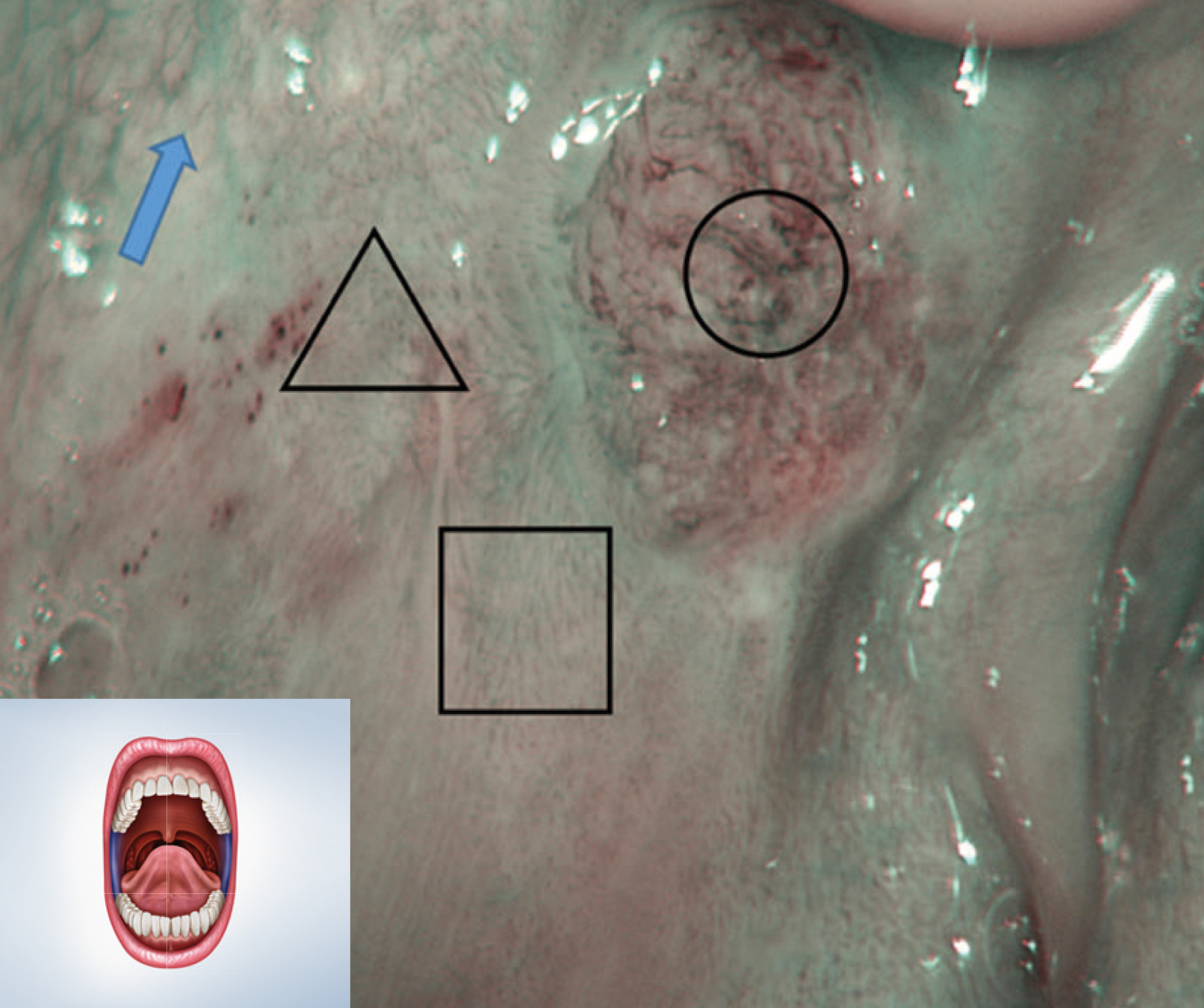
Retromolar trigone labial and buccal mucosa, dysplastic pattern.

Posterior left buccal mucosa. The area with high-grade dysplasia is visible as an image resembling a honeycomb mesh made of multiple polygonal areas (〇). In the dysplastic area the submucosal large light-blue vessels are no longer visible, but can be glimpsed in the surrounding areas (thick light-blue arrow). Superficial mucosal capillaries are still visible as short dashes (black thin arrow) outside the dysplastic area.
Type 1 Epithelium
Neoplastic Pattern
Gingiva, hard palate and dorsal surface of the tongue, neoplastic pattern.
Right hard palate. Neoplastic vessels have a completely altered structure; they appear as dark-green dilated winding vessels at the tumor limits (〇); conversely they are not visible in necrotic areas (▢).
Type 2a Epithelium
Neoplastic Pattern
Floor of the mouth and ventral tongue, neoplastic pattern.
Left tongue margin. Neoplastic vessels have a completely altered structure; they appear as dark-green dilated winding vessels (〇); conversely they are not visible in necrotic areas (▢).
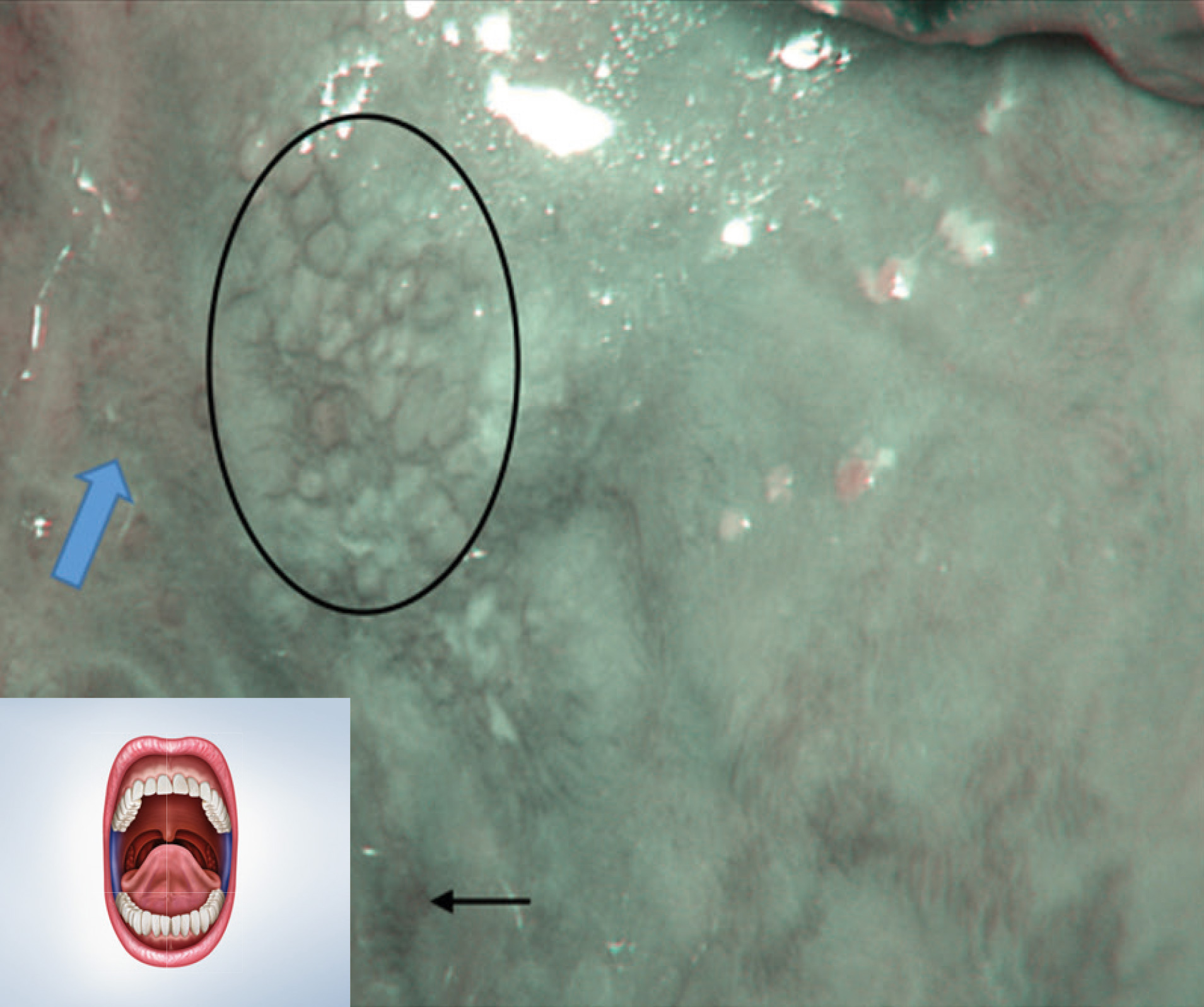
Type 2b Epithelium
Neoplastic Pattern
Retromolar trigone, labial and buccal mucosa, neoplastic pattern.

References
Lin, Y.C., Wang, W.H., Lee, K.F., Tsai, W.C., and Weng, H.H. (2012). Value of narrow band imaging endoscopy in early mucosal head and neck cancer. Head and Neck, 34, 1574-1579. doi: 10.1002/hed.21964
Tirelli, G., Marcuzzo, A.V., Boscolo Nata, F. Narrow-band imaging pattern classification in oral cavity. Oral Dis. 2018; 24(8): 1458-1467. doi: 10.1111/odi.12940
Boscolo Nata, F., Tirelli, G., Capriotti, V., et al. NBI utility in oncologic surgery: An organ by organ review. Surg Oncol. 2020; 36: 65-75. doi: 101016/j.suronc.2020.11.017
Tirelli, G., Piovesana, M., Gatto, A., et al. Narrow band imaging in the intra-operative definition of resection margins in oral cavity and oropharyngeal cancer. Oral Oncol. 2015; 51(10): 908-13. doi: 10.1016/j.oraloncology.2015.07.005
Tirelli, G., Piovesana, M., Gatto, A., et al. NBI utility in the pre-operative and intra-operative assessment of oral cavity and oropharyngeal carcinoma. Am J Otolaryngol. 2017; 38(1): 65-71. doi: 10.1016/j.amjoto.2016.09.020
Tirelli, G., Piovesana, M., Marcuzzo, A.V., et al. Tailored resections in oral and oropharyngeal cancer using narrow band imaging. Am J Otolaryngol. 2018; 39(2): 197-203. doi: 10.1016/j. amjoto.2017.11.004
Tirelli, G., Piovesana, M., Gatto, A., et al. Is NBI-Guided Resection a Breakthrough for Achieving Adequate Resection Margins in Oral and Oropharyngeal Squamous Cell Carcinoma? Ann Otol Rhinol Laryngol. 2016; 125(7): 596-601. doi: 10.1177/0003489416641428
Tirelli, G., Piovesana, M., Gatto, A., Boscolo Nata, F. Narrow-band imaging with 4K technology in the head and neck: preliminary experience and technical settings. Br J Oral Maxillofac Surg. 2017; 55(7): 740-741. doi: 10.1016/j.bjoms.2017.06.009
Tirelli, G., Piovesana, M., Bonini, P., Gatto, A., Azzarello, G., Boscolo Nata, F. Follow-up of oral and oropharyngeal cancer using narrow-band imaging and high-definition television with rigid endoscope to obtain an early diagnosis of second primary tumors: a prospective study. Eur Arch Otorhinolaryngol. 2017; 274(6): 2529-2536. doi: 10.1007/s00405-017-4515-x